 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
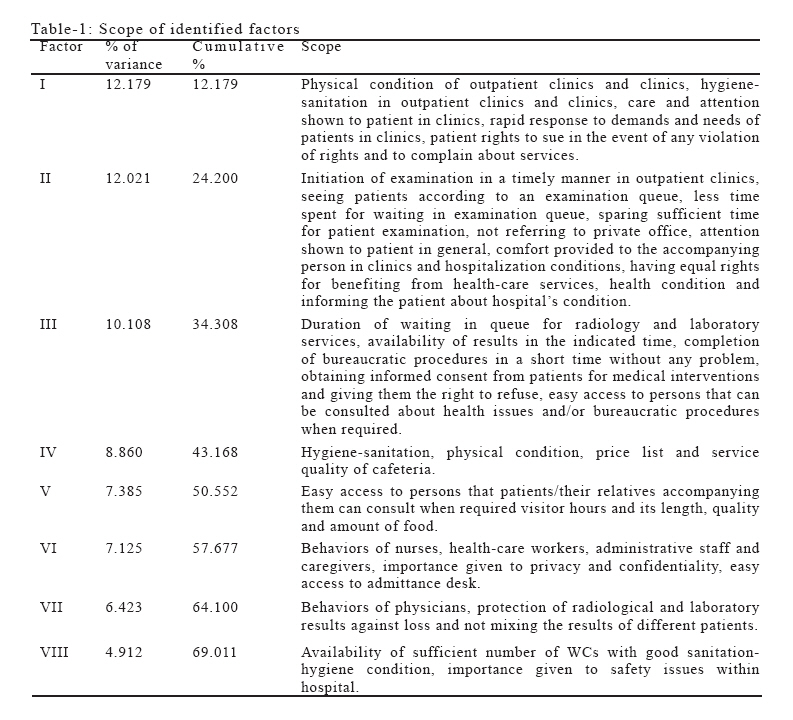
European Journal of General Medicine, Vol. 3, No. 2, 2006, pp. 73-77 ALGORITHM FOR INCREASING PATIENT SATISFACTION RELATED WITH NON-TECHNICAL DIMENSION OF SERVICES IN TURKEY İlker Ercan1, Güven Özkaya1, Züleyha Alper2, Bülent Ediz1, Emine Özgür Bayman3, İsmet Kan1, Nazan Bilgel2 Uludag University, Faculty of Medicine, Departments of Biostatistics1 and Family Medicine2, Bursa, Turkey, University of Iowa, School of Public Health, Department of Biostatistics3, Iowa, USA Correspondence: Dr. Ilker ERCAN, Uludag University, Faculty of Medicine, Department of Biostatistics, Gorukle Campus, 16059, Bursa, Turkey Phone: 902244428200 (21028), Fax: 902244428666 E-mail:ercan@uludag.edu.tr Code Number: gm06015 Aim: In this study, a guiding algorithm aiming to increase patient satisfaction related with non-technical dimension of services at not gain-aimed secondary health care-services in developing countries like Turkey is searched. Key words: Satisfaction, Health Service, Management, Factors, Algorithm INTRODUCTION In medicine, a practical science, research and practices are performed on medical issues such as diagnosis of physical and mental disorders in humans, prescription of drugs for these disorders, medical or surgical interventions and administration of therapeutic methods. During practice, health-care provider and the patient, demanding health-care services interact in the same setting. Satisfaction or dissatisfaction resulting from the individuals or setting may be encountered during this interaction (1). Consumers personally participate in the productive process in service organizations. Thus, consumer satisfaction is important in such organizations. The same applies also for consumers of health-care services (2). Patient satisfaction is an important part of quality service (2). Patients’ perceptions about health care systems seem to have been largely ignored by health care managers in developing countries (3). Determination of patient satisfaction levels is critical for improving the quality of services and providing more sophisticated services fulfilling the expectations of patients (4). A patient who is satisfied with the provision of health-care services in a facility, would admit to the same facility when he/she seeks medical attention (2). While the goods are defined as “an object, a tool or matter”, services imply “an activity, a performance or effort”. Thus, it is more difficult to assess a qualitative term like “service” than to assess goods which is a quantitative term (2). Quantitative measurements are measurements performed with a physical tool. However measurement of attitudes or opinions has a qualitative aspect because it does not involve a physical measuring tool (1). In order to address daily problems encountered during production in advance and to evaluate and improve services, research on services should be carried out. To achieve this, educational and research administrations should collaborate with health-care organizations and undertake responsibility and appropriate funds should be spared for research on services (5,6). Data about patient opinions obtained by systematical follow-up of consumers of health-care resources would be a valuable guide towards improving quality of services (7). In order to obtain information about and improve quality of health-care system, major variables of interest such as extent of service use, percentage of attainment and satisfaction scores should be assessed (7-9). Statistical methods are required to measure and assess these variables accurately. While measuring satisfaction from services, information on cognitive and emotional behaviors of individuals is sought. Because such behavioral patterns have qualitative features, they do not bear the easiness of measurement conferred by quantitative features. A Scale designed to measure qualitative features should consist of a sample of items that best represents the behavioral pattern which is desired to be measured and should be least confounded by bias sources. Associations have to develop proper methods in order to measure and improve satisfaction level. One of these methods is to make patient satisfaction investigations aiming to determine dissatisfaction sources in order to remove knowledge deficiency. Investigation results show that hospitals that are not gain-aimed are also interested in patient satisfaction and 79% of them make investigations aiming to measure patient satisfaction (4). This study is performed in order to guide secondary health care services which regard satisfaction-aimed management policy but can not make investigations in order to measure patient satisfaction. The results of this study are expected to guide managers of health-care systems at their studies aiming to increase patient satisfaction related with non-technical dimension of services in developing countries like Turkey. MATERIAL AND METHOD Implementation of scale: The scale which was developed and, reliability and validity analyses were done by Ercan et. al (10), was applied to measure non-technical dimension of service satisfaction from services provided by a secondary health-care unit. The scale developed by Ercan et. al (10) in order to measure patient satisfaction in associations that are in secondary health-care services include components evaluating clinical-policlinical health care services, staff, patient-rights, hospital appearance, cafeteria services . This research was performed in Zubeydehanim Gynecology and Obstetric Hospital, Bursa-Turkey. During implementation, benefiting from health-care services of that hospital at least once was required. Implementation of the study was lasted for one year and including face-to-face interview with subjects. Scale was applied to 173 subjects and afterwards reliability analysis was done with cronbach alpha. Performing Factor Analysis: Three items of scale related to general evaluation were excluded from factor analysis. Factor analysis was performed to form groups of unrelated items by gathering related items in the scale and to rank factors affecting satisfaction by their importance (11). Kaiser-Meyer-Olkin measure of sampling adequacy and Bartlett’s test of sphericity were performed on data set in order to assess appropriateness for factor analysis. Homogeneity of variances in variables was tested by Levene statistics to determine the data matrix which will be used in factor analysis. First, factor analysis was performed without rotating the axes. After observing that the variables were distant to axes, varimax method was considered as the best rotation among orthogonal rotation methods for our data set following application of several rotation methods. When performing factor analysis, factor selection was done by considering number of eigenvalue greater than 1. The SPSS 12.0 software was used for statistical analyses. RESULTS Cronbach alpha was determined as α=0.9682, so scale was considered as reliable. Before performing factor analysis Kaiser-Meyer-Olkin measure of sampling adequacy (KMO=0.909) and Bartlett’s test of sphericity (χ2=4937.26, υ1=903, p<0.001) were done. Homogeneity of variances in variables was tested by Levene statistics (Levene statistics=13.605, υ1=11, υ2=1776, p<0.001). After performing tests we decided that factor analysis could be applied on our data set and that use of correlation matrix computed by raw data matrix in the analysis was appropriate (12-14). By using varimax rotation method, 8 factors were defined by considering number of eigenvalue greater than 1. Factors identified would solve the problem by a rate of 69.01% explaining general variance in order to improve satisfaction from health-care services. Scope of identified factors and their rate of explaining general variance were shown in Table 1. DISCUSSION Patient satisfaction differentiates according to socioeconomic, demographic, functional conditions and health (4, 15, 16-18). In this study, it is not concentrated on these features affecting patient satisfaction because the aim of the study is to form an algorithm in order to increase patient satisfaction related with non-technical dimension of services that aims to guide secondary health-care services that can not make investigations aiming to measure patient satisfaction. For this reason, factors that can help guiding system managers (managers adopting satisfaction-aimed management policies) in their first approaches or in impossible conditions to make investigations aiming patient satisfaction are tried to be determined according to their importance. According to the results of our study an eight-staged algorithm is suggested to system managers in their studies aiming to increase patient satisfaction related with non-technical dimensions. In first stage, matters that have to be dealed up in studies aiming to increase patient satisfaction are physical conditions of clinics and outpatient clinics, cleanliness and hygiene of clinics and outpatient clinics, interest and care in the clinic, meeting health needs and carrying out health requests quickly, giving patients request rights about any services and complaints right in unfair conditions. So, matters that have to be dealed up include mostly outpatient clinics and clinic conditions in first stage. In second stage, matters that have to be dealed up in studies aiming to increase satisfaction are starting the examination in outpatient clinics at the right time, examining patients as to their turns, shortage of turn awaiting times, spending enough time for patients, doctors’ behaviour of guiding patients to their offices outside the hospital, the general interest, comfort of patient companions and hospitalisation conditions in clinics, benefiting of every patient from care services equally, informing patients about their health and hospital possibilities. So, matters that have to be dealed up in order to increase satisfaction include mostly time in second stage. Matters that a system manager has to deal up in order to increase satisfaction in third stage are turn awaiting times at laboratory and radiology services, giving results at the determined time, finishing the bureaucratic procedures in a short time with no problem, performing operations with approvals and giving a refusal right, patient’s finding a competent to consult about matters related with bureaucratic procedures easily. So, matters that have to be dealed up in order to increase patient satisfaction include again mostly time related with laboratory, radiology services and bureaucratic procedures in third stage. Matters that a system manager has to deal up in order to increase satisfaction in fourth stage are cleanliness, hygiene, physical conditions, prices and service quality of cafeteria. So, in this stage matters are mostly related with cafeteria. Matters that a system manager has to deal up in order to increase satisfaction in fifth stage are finding of patients/companions a competent in order to get information in the clinic easily, patient visiting hours and periods, quality and amount of foods given to patients. Matters that a system manager has to deal up in order to increase satisfaction in sixth stage are behaviours of nurses, other health-aid staff and administrators, attaching importance to secrecy and privacy, finding the first information desk easily in the hospital. So, matters that have to be dealed up include mostly behaviours of staff in this stage. Matters that a system manager has to deal up in order to increase satisfaction in seventh stage are behaviours of doctors, not being mixed or not being lost of results at radiology and laboratory services. So, matters that have to be dealed up include mostly the results of radiology and laboratory services in this stage. Matters that a system manager has to deal up in order to increase satisfaction in last stage are having enough number of clean and hygienic toilets in the hospital. When we examine the similar studies about patient satisfaction by also taking our study in to consideration, it is seen that the time spent at health-care service, behaviours of staff, cleanliness and hygiene, food quality and cafeteria services have important effects on patient satisfaction related with non-technical dimensions of health services (3,17,19-23). It is seen in our study that components related with time especially have important effect on patient satisfaction. Although in order of priorities some items have concordance with each other according to content, some items have discordance. The reason is that service requesters can not determine the priorities clearly for themselves because quality consciousness of patients develops not enough in health services. This situation causes difficulties in planning of health services focused satisfaction in developing countries like Turkey. By means of our study, we present an algorithm to system managers of not gain-aimed secondary health care services in Turkey that will be useful in their studies aiming to increase patient satisfaction related with non-technical dimension of services. The perception of satisfaction differentiates between people, community, and health care systems surely (16-18,22,24-26). If conditions different from community features and present health care systems exist, there will be changes in importance sequence of components affecting patient satisfaction. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06015t1.jpg] |
| |||||||||

{kind=link}