 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
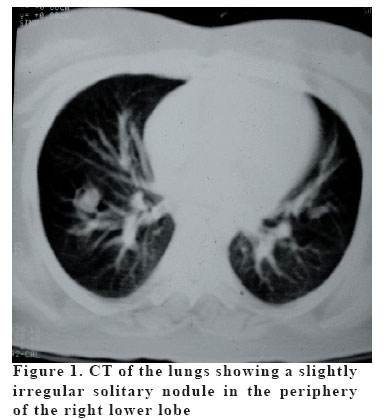
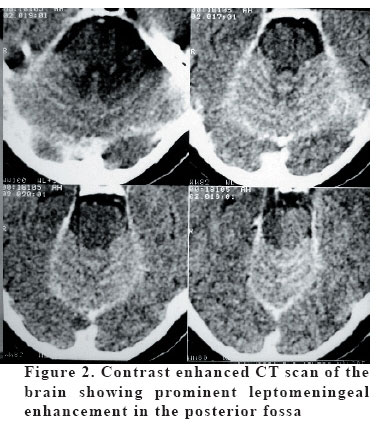
European Journal of General Medicine, Vol. 3, No. 2, 2006, pp. 80-82 CRYPTOCOCCAL MENINGITIS AND PULMONARY CRYPTOCOCCOSIS IN A NON-HIV INFECTED PATIENT Lekha Pandit1, Amit Agrawal2, Shalini Shenoy3, Ganesh Kamath4 K.S. Hegde Medical Academy, Professor of Neurology1, Associate Professor of Neurosurgery2 Kasturba Medical College, Professor of Microbiology3, A.J. Shetty Medical College, Associate Professor of Radiology4 Correspondence: Dr Amit Agrawal ,Associate Professor of Neurosurgery, Department of Neurosurgery, K.S. Hegde Medical Academy, Nityananda Nagar, Mangalore-575108, Karnataka,India. E-mail: dramitagrawal@gmail.com Code Number: gm06017 Pulmonary cryptococcosis associated with cryptococcal meningitis in non-HIV infected patients is an uncommon finding. We report a case of polymyositis who developed pulmonary cryptococcosis and cryptococcal meningitis while she was on long term oral steroids, treated successfully. Key words: AIDS, Cryptococcus meningitis, HIV, immunosuppressive therapy INTRODUCTION Cryptococcosis has dramatically increased in frequency as a result of the pandemic of human immunodeficiency virus (HIV) infection and an enlarging population of other immunocompromised individuals (1,2). Pulmonary cryptococcosis associated with cryptococcal meningitis in non-HIV infected patients is an uncommon finding (3,4). Amphotericin B, fluconazole, and amphotericin B in combination with flucytosine have been used in the treatment of cryptococcal meningitis with and without coexisting HIV infection with significant improvements in the management of cryptococcal meningitis (1). In present case report, the patient was on long term oral steroids for polymyositis than she developed pulmonary cryptococcosis and cryptococcal meningitis that was treated successfully. CASE Nineteen year old female, a muscle biopsy proven case of polymyositis, was on long term treatment with oral prednisolone (1.5 mg/kg body weight) and Azathioprine (50 mg/day) presented with history of fever associated with productive cough of 2 weeks duration followed by increasing headache and drowsiness of 1 week duration. On examination she was febrile (101.6 degree F), pulse rate was 96/min, and BP-110/70 mmHg. Auscultation of chest revealed diminished breath sounds with crepitations in right infra mammary and infra axillary area. Neurologically she was drowsy and there was neck stiffness. Fundus examination showed bilateral papilloedema. There were no other focal neurological signs. Routine investigations revealed an Erythrocyte sedimentation rate of 110mm/hr; total count was 11,000/cu mm, differential count was Neutrophils-64%, Lymphocytes-34% and Eosinophils-2%. Chest X-Ray and CT (Computerized tomography) (Figure-1) of chest showed a nodular opacity in the right lower lobe of the lung that was enhancing after contrast administration. CT scan head showed prominent leptomengial enhancement especially in the posterior fossa (Figure-2). India ink staining of sputum was positive for Cryptococcus. Cerebrospinal fluid (CSF) analysis revealed 450 cells, predominantly lymphocytes, with protein of 110 mg/dl and glucose of 23 mg/dl (corresponding blood glucose- 110 mg/dl). India ink staining and fungal culture was positive for crypococcus neoformans. Patient was started on intravenous Amphotericin B (0.7 mg/kg /day) and oral fluconazole 200 mg every 8th hourly. Amphotericin B was stopped after 2 weeks however oral flucanazole was continued in spite of two negative CSF smear and culture for cryptococcus for a further six weeks. At follow up after 24 months, she remains well on 20 mg alternate day dose of oral prednisolone. She also delivered a healthy baby two months ago. DISCUSSION Cryptococcus neoformans is a yeast, most commonly infects the central nervous system. Resistance to cryptococcosis depends primarily on cell-mediated immunity. Therefore, most cases of cryptococcal meningitis occur in patients with conditions that weaken this system, such as AIDS. Cryptococcal meningitis has also been sporadically reported in HIV negative patients in the background of organ transplant and chemotherapy related immunosuppression, reticuloendothelial malignancies, corticosteroid therapy and sarcoidosis (3, 6). Occasionally no obvious underlying cause can be detected (5, 6). Our patient’s clinical presentation coupled with high ESR and CSF cytochemistry strongly suggested the diagnosis of pulmonary tuberculosis and tuberculous meningitis. However the lung lesion was atypical for pulmonary tuberculosis and this alerted us to investigate for alternate causes particularly when this patient was long term steroids (1). Several unique features differentiate cyptococcal meningitis seen in HIV positive patients from those with HIV negative states. Cryptococcal pneumonia, the symptoms of which include cough, fever, and infiltrates or mass in the lungs have been previously reported among people with chemotherapy or organ-transplant-related immunosuppression, but not among people with AIDS (7). Leptomeningeal enhancement on CT (as in present case) and magnetic resonance imaging (MRI) studies secondary to cryptococcal meningitis is an uncommon finding. Significant differences are reported in the inflammatory response to cryptococcal meningoencephalitis among patients with and those without HIV infection (8, 9). Brisk response to therapy, negative smear and cultures after a short period of antifungal therapy and the non-requirement of long term maintenance treatment are more commonly seen in cryptococcal meningitis affecting non-HIV infected patients (1,10). The prominent clinical symptoms and signs of meningitis, increased intracranial pressure, reactive CSF and brisk response to therapy in our patient all support these observations. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06017f1.jpg] [gm06017f2.jpg] |
| |||||||||

{kind=link}
{kind=link}