 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
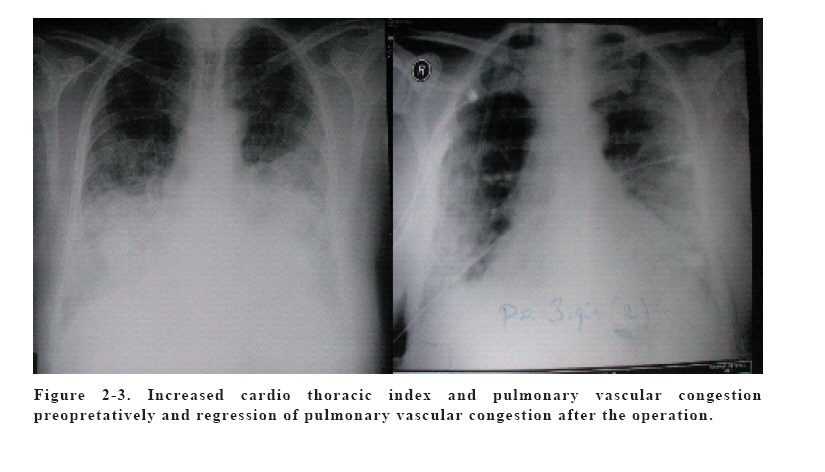
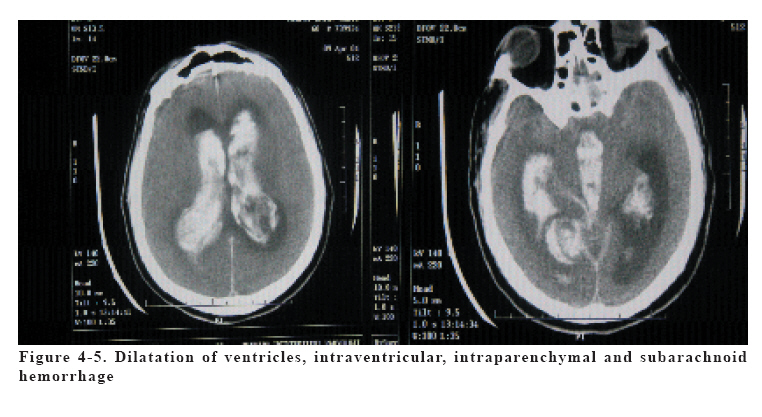
European Journal of General Medicine, Vol. 3, No. 2, 2006, pp. 83-87 STREPTOCOCCUS BOVIS ENDOCARDITIS ASSOCIATED WITH RECTAL CARCINOMA AND ITS NEUROLOGICAL COMPLICATIONS Yasin Abul1, Zekaver Odabasi2, Nihat Kodalli3, Ahmet Oktay4, Volkan Korten2 Marmara University School of Medicine, Internal medicine, Departments of Pulmonary and Critical Care Medicine1, Infectious Diseases2, Radiology3 and Cardiology4, İstanbul, Turkey Correspondence: Yasin Abul, MD. Marmara University Hospital, Department of Pulmonary and Critical Care Medicine, Tophanelioglu caddesi, No:13, 81190, Altunizade, Istanbul, Turkey Phone 902163262162 Fax: 902164280335 E-mail: abulyasin@yahoo.com Code Number: gm06018 Infective Endocarditis caused by Streptococcus bovis may usually be associated with gastrointestinal pathologies, particularly colon cancer. S. bovis endocarditis may cause higher rates of neurological complications and more extensive valvular destruction compared to other microorganisms. This case report describes a patient with a recent history of rectal adenocarcinoma diagnosed as S. bovis endocarditis and complicated by intracranial and subarachnoidal hemorrhage after cardiac valve replacement. Because of high rates of neurological complications, these patients should be carefully followed up even after the medical and/or surgical treatment. Key Words: Endocarditis, bacterial, Streptococcus bovis rectal carcinoma, intracranial hemorrhage, subarachnoid hemorrhage, valvular destruction INTRODUCTION Streptococcus bovis endocarditis is the second most common cause of all streptococcal endocarditis cases; it may be associated with gastrointestinal pathologies, particularly colon cancer (1,2,3). Association between colon cancer and presence of infective endocarditis was described in 1951 (4). Streptococcus bovis endocarditis has a more common involvement of multiple valves, and more common occurrence of hemodynamically relevant valvular regurgitation requiring cardiac surgery for 70 to 73% of patients(5,6). Also neurological complications are more frequently seen in Streptococcus bovis endocarditis(5,7). This study presents a case report of Streptococcus bovis endocarditis associated with rectal carcinoma complicated by extensive valvular involvement and also intracranial, subarachnoid hemorrhage after cardiac valve replacement. CASE A 62-year-old man with hypertension and a recent history of rectal adenocarcinoma (Figure 1) presented to our clinic with exertional dyspnea, orthopnea, pretibial edema, fever and malaise. He had colonic resection and adjunctive postoperative chemotherapy 5-fluorouracil and radiotherapy, six weeks before his admission. He had a history of cardiac failure stage A and it was progressed to stage D during postoperative period. A low grade fever was started 4 weeks after his operation and it was gradually increased to 39,5ºC three days before his admission. In his physical examination in Emergency Department, cardiac sounds could not be clearly heard due to tachypnea and pulmonary rales. His electrocardiogram was normal except right bundle branch block and sinus tachycardia of 105 beats/min and there were no ischemic changes. Troponin-T test was positive in low titers and he had no chest pain. His blood pressure was 150/60 mm Hg, body temperature was 37,2ºC, respiratory rate was 32/minute. There were remarkable pulmonary rales up to the middle chest levels, a 2/6 systolic murmur along the apex and 1-2/6 diastolic murmur at the right second intercostal area and profuse pretibial edema. Chest X-Ray revealed increased cardio thoracic index and pulmonary vascular congestion (Figure 2). Complete blood count showed leukocytosis (14,700/µl) and anemia (10,4 g/dl). Arterial blood pH was 7,45, partial oxygen saturation was 50,5 mmHg. Trans thoracic echocardiography revealed vegetations on both the aortic and mitral valves with dimensions of 20x11 mm and 11x8 mm respectively. Significant aortic insufficiency (grade 4) and mitral insufficiency (Grade 4) were also detected. The left ventricle was slightly increased in size and left ventricle ejection fraction was 50%. Fundoscopic examination for ocular manifestation of infective endocarditis was negative. The clinical diagnosis was infective endocarditis and Stage D congestive cardiac insufficiency and the patient was transferred to the coronary care unit. His rhythm was atrial fibrillation. His medical treatment was regulated for the congestive heart failure and atrial fibrillation. For the empirical treatment of infective endocarditis gentamycin 2x80 mg IV, cefazolin 3x2 g IV, and ampicillin 4x3 g IV was applied for the coverage of streptococcus bovis endocarditis. During the follow up, patient’s clinical picture deteriorated and pulmonary rales progressed up to upper lung levels. His respiratory rates, increased up to the 50/min. His cardiac rhythm returned to the sinus but because of his progressive heart failure caused by significant aortic insufficiency, the patient underwent aortic and mitral valve replacement . Both aortic and mitral valves were replaced. In addition to the aortic and mitral valve vegetations, another vegetation of the posterior wall of the ascending aorta was also recognized during operation. His body temperature elevated to the 38 ºC at postoperative 2nd day. Blood and tissue culture showed coagulase negative S. bovis, which was sensitive to penicilin-G (MIC=0,064). His antimicrobial therapy was continued as gentamycin 2x60 mg IV and Ampicillin 4x2 gr IV postoperatively. His inotrops was stopped at the 6th day postoperatively Pulmonary findings on radiogram was regressed (Figure 3). He had no fever and his clinical picture was improved during the inpatient ward follow up. But he developed sudden onset of tachypnea, tachycardia and decreased consciousness at postoperative 15th day. His blood pressure 220/110 mmHg, at that time his eyes was fixed , respiration was paralyzed and the patient suddenly collapsed, He was immediately entubated and transferred to the medical intensive care unit. Neurological examination showed pupillary anisocoria with miotic right pupil (1mm), mydriatic left pupil (5 mm); corneal , oculocephalic and light reflexes was not detected and his Glascow Coma Scale was 3 point at Intensive Care Unit presentation. Cerebral computed tomography showed dilatation of ventricles, intraventricular hemorrhage, intraparenchymal hemorrhage and subarachnoid hemorrhage (Figure 4-5). His INR was 2,34 and subtherapeutic. Dexamethasone treatment was administered to the patient. The patient was evaluated as intraventricular hemorrhage and acute hydrocephaly. But his brain stem reflexes was absent and he was accepted as inoperative. Twenty days after the operation of vulvular replacement, pupils widened acutely and became unreactive bilateraly. The patient died on the same day. DISCUSSION S. bovis can be found in the normal flora of human gastrointestinal system. It is classified in non-enterococcal Streptococcus species particularly Lancfield’s group D. It is the second common Streptococci causing bacterial endocarditis. Other common streptococci isolates causing infective endocarditis are Streptococcus sanguis, Streptococcus mutans, and Streptococcus mitis (1,3). S. bovis endocarditis is often associated with colon and polyps as adenocarcinoma. In some studies from USA, colon adenocarcinomas were mostly associated with S. Bovis endocarditis, although some others showed it is more common with benign tumors (2,8,9,10). Possible gastrointestinal source has been found in up to 84% of cases (1,11). S. bovis endocarditis generally affect the elderly patient population over 60 years of age (6,12,13). Colonic tumors may be detected after the diagnosis of infective endocarditis or patients of S. bovis endocarditis may have a history of colonic neoplasia like our patient (9,14,15). Other gastrointestinal diseases associated with the S. bovis endocarditis are gastric ulcers, gastric cancer, duodenal ulcers, inflammatory bowel disease, colonic diverticula, angiodysplasia and liver cirrhosis(6). Up to 56% of patients with S. bovis endocarditis have concomittant gastrointestinal tumors which was not diagnosed previously(8). The most common clinical manifestations of S. bovis endocarditis are fever and malaise like on our patient. S. bovis endocarditis may also be presented as Stage D heart failure and conduction abnormalities like right bundle branch block (15) which was also present in our patient. S. bovis endocarditis causes multiple and more extensive valvular damage than the endocarditis caused by other microorganisms as in our patient having mitral and aortic valve involvement and also aortic root vegetation (6,15,16). S. bovis endocarditis involves mostly the multiple valves simultaneously and causes hemodynamically unstable valvular insufficiency which usually necessitates cardiac surgery in up to 73% of patients.(5,6,15). Additionally S. bovis endocarditis has a worse long term prognosis than infective endocarditis caused by other microorganisms(6) In general, neurologic manifestations of the infective endocarditis in all microbiological species includes thromboembolic brain infarction , transient ischemic attack , cerebral hemorrhage, meningitis, brain abcesses, toxic encephalopathy, and headache(17). The incidence of stroke in S. bovis endocarditis is around 6% (15). Higher rates of valvular destruction, thromboembolic events, and neurological complications are seen in S. bovis endocarditis (5,6,15). Ischemic stroke and splenic rupture that are both due to thromboembolism in S. bovis endocarditis described in literature (18). S. bovis endocarditis may cause subarachnoid hemorrhage which is most commonly resulted from rupture of mycotic aneurysm. Also pyogenic arterial wall necrosis due to septic embolism may cause subarachnoid hemorrhage in S. bovis endocarditis apart from the rupture of mycotic aneurysm. These two mechanisms should be distinguished from each other (19). Even though patients with S. bovis endocarditis is treated medically and surgically, mycotic aneursyms or pyogenic arterial wall necrosis may progress to subarachnoid hemorrhage and may cause mortality in long term prognosis. Because short and long term neurological complications may be seen commonly in S. bovis endocarditis, these patients should be evaluated and followed carefully. Further radiodiagnostic investigations should be considered in S. bovis endocarditis. In conclusion, compared to other Streptoccal endocarditis, S. Bovis endocarditis has more destructive cardiac and neurological complications. Team work including emergency medicine, cardiology, cardiovascular surgery, microbiology, infectious diseases, gastroenterology and critical care medicine departments are required for rapid diagnosis and treatment. Because neurological complications cause serious mortality and morbidity even after the treatment, patients with S. bovis endocarditis should be evaluated in details about the neurological complications. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06018f1.jpg] [gm06018f4-5.jpg] [gm06018f2-3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}