 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
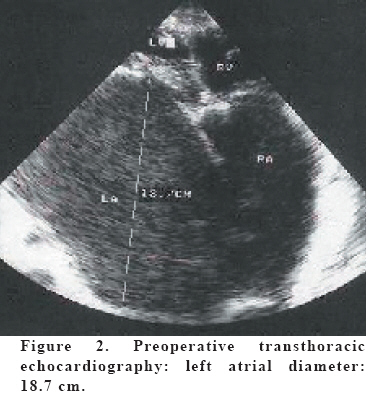
European Journal of General Medicine, Vol. 3, No. 2, 2006, pp. 90-92 HUGE LEFT ATRIUM Mehmet Ateş¹, Yavuz Şensöz¹, Günseli Abay¹, Murat Akçar¹ Siyami Ersek Thoracic and Cardiovascular Education and Research Hospital, Departments of Cardiovascular Surgery1 and Anesthesiology and Reanimation2 , İstanbul, Turkey Correspondence: Mehmet ATES, Merdivenkoy Mah. Sairarsi Cad.Emincinarpasa Sok. No:6 Dicle Apt. D:24 Goztepe/Kadıköy, İstanbul, Türkiye Tel-Fax: 902163600272, Mobile Phone: 905337442452 E-mail:drmates@yahoo.com Code Number: gm06020 Chest X-ray examination of a 38-years-old female patient, who was diagnosed as having mitral stenosis, revealed cardiac enlargement due to huge left atrium. Cardiothoracic ratio was approximately 0.90. Cardiac enlargement was due to the distortion of cardiac structures by giant left atrium. Giant left atrium can be readily demonstrated by echocardiography. Delaying the operation for mitral valve replacement may lead to fatal outcomes. Optimal timing for operation is important in mitral stenosis. Key words: Huge left atrium, mitral stenosis, echocardiography INTRODUCTION Left atrium dilates and hypertrophies in mitral stenosis cases. Occasionally left atrium reaches to extreme sizes. In giant left atrium cases, mitral stenosis may be the sole pathology or it may be accompanied by mitral insufficiency, or it may present as mixed mitral disease where mitral stenosis dominate. Transthoracic echocardiography is the easiest and cheapest method for the diagnosis and follow-up of the disease. Transesophageal echocardiography performed during the operation helps the surgical team in evaluating the effectiveness of artificial valves (1). CASE A 38 years old female patient was admitted to our institution with dyspnea and palpitation. These complaints had been present for the last four years but worsened for the last 15 days. She had been diagnosed with rheumatic heart disease 4 years ago by echocardiography revealing a mitral valve area of 0.5 cm2 and a left atrial diameter of 10 cm. According to these findings she had been offered operation but she refused operation and she had been taking medical treatment. Transthoracic echocardiography demonstrated a mitral valve area of 0.3 cm2, 3 (+) mitral insufficiency and 3-4 (+) tricuspid insufficiency. Left atrial diameter was 18.7 cm. We tried to manage the advanced heart failure and stabilize the patient. However her dyspnea continued despite 7 days of medical treatment. Upon obtaining necessary consent from the patient and the family, we decided to operate her. Her physical examination revealed the following findings: BP was 80/40 mmHg, heart rate was 110/min and AF, neck veins were distended, crepitations were present at the basal regions of lungs, diastolic murmur and 3-4(+)pansystolic murmur were present on midclavicular line, there were 2(+) peripheral edema and the patient was evaluated as NYHA-IV. Electrocardiography showed atrial fibrillation, right ventricular enlargement Telecardiography demonstrated massive cardiomegaly, pleural fluid in both hemithoraxes (Figure 1). Echocardiography revealed a left atrial diameter of 18.7 cm and a valvular area of 0.3 cm2. Maximal gradient was 30 mmHg. and LVEF was 40% (Figure 2). Operation and postoperative period: Patient was operated in this status and could only be intubated in almost sitting position, and Swan-ganz catheter was placed. Central venous pressure was 18 mmHg, pulmonary artery pressure was 65/35 mmHg, and systemic blood pressure was 80/50 mmHg. Wedge pressure could not be measured. Under general anesthesia, mediastinum was opened via midsternal incision, pericardium was opened, and cardiopulmonary bypass was commenced by the cannulation of superior vena cava, inferior vena cava and aorta. Cross clamp was placed. Cardiac arrest was provided by 33ºC systemic hypothermia and antegrade blood cardioplegia. Following right atriotomy, severe insufficiency of tricuspid valve was observed. Left atrium was entered through atrial septum and advanced fibro-calcification of mitral valve was found. Mitral valve was resected with preservation of posterior mitral leaflet and a no 31 St-Jude mechanical valve was replaced. Organized thrombus of 1-2 cm diameter, which was adhered to left atrial wall, was removed and 5 cm. left atrial plication was performed, left atrial appendix was ligated internally with 5/0 prolene suture material. De-Vega annuloplasty (no 33) was done for the tricuspid valve. Cross-clamp time was 62 min., cardiopulmonary bypass time was 105 min. She was transferred to postoperative intensive care unit with medical support. Drainage tubes were removed on the first postoperative day and she was extubated on the same day. However she was re-intubated on the second postoperative day due to dyspnea. Tracheostomy was performed on the fifth day; she had hypotension and bradycardia on the 10th. day, she did not respond to cardiopulmonary resuscitation and died. DISCUSSION Delaying the operation for mitral valve replacement may lead to fatal outcomes. Sinatra et al. reported a 56 years old male case with a left atrial diameter of 17 cm. measured by echocardiography. Magnetic resonance imaging revealed a left atrial size of 18x20x17 cm. for the same patient (1). Due to the clinical status of our patient, we could not perform magnetic resonance imaging. Left atrial diameter of 17 cm. reported by Riccardo and colleagues was the largest diameter that we could find in the literature. Therefore, we consider the left atrial diameter of 18.7 cm. that we found in our case as the largest left atrial diameter reported to date. Optimal timing may be life saving in mitral valve operations. In delayed cases, increased pulmonary artery pressure contributes to the increase in pressures of the right side. Thus, it unfavorably affects mortality and morbidity rates (2). In the review of Hurst, it is stated that, in giant left atrium cases, mitral regurgitation is more profound than mitral stenosis, atrial fibrillation is almost always present, chest x-ray may reveal pleural fluid and dysphasia may be present. Our patient could not cooperate well, so we obtained her history from relatives, which revealed that she had had dysphasia. In these cases, pulmonary edema and dyspnea are also observed due to increased pulmonary pressure. In USA, same cases were reported until the end of 40’s, however today giant left atrium cases are not frequently reported from this country. Few cases are the immigrants from outside of USA (2). According to the definition of Isomura et al., left atriums of grater than 6 cm diameter are giant left atriums (3) We suggest that left atriums with a diameter above 10 cm should be regarded as giant left atriums in our country where rheumatic heart diseases are common; left atriums of a diameter between 6-10 cm however, should be considered as left atrial enlargement. Johnson et al. proposed that left atrial enlargement is not solely due to mitral regurgitation, but left atrial wall is also responsible (4). Lessana et al. (5) described auto transplantation techniques for effectively decreasing the size of left atrium. In this technique, following cross-clamping, superior vena cava, aorta and pulmonary artery are detached and the heart is easily moved upwards. Left atrial diameter is resected until it is decreased to 5 cm. Mitral valve replacement is performed at this position and pulmonary artery, aorta and vena cava are re-anastomosed. In our case, left atrial plication was done and 18.7 cm. of preoperative left atrial diameter could be decreased to 13.3 cm. postoperatively (5) As our case was in terminal stage, as mitral stenosis was more profound than mitral insufficiency, and due to advanced pulmonary hypertension and emergent operative conditions, our mortality risk was high. We wished to report the left atrium with 18.7 cm. of diameter, which is the largest atrium reported to date, despite the fatal outcome. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06020f1.jpg] [gm06020f2.jpg] |
| |||||||||

{kind=link}
{kind=link}