 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
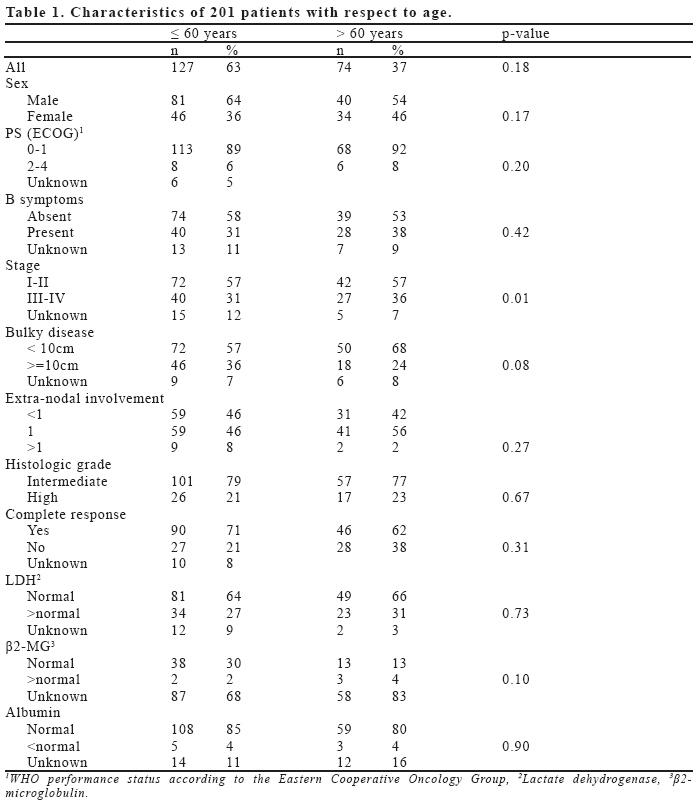
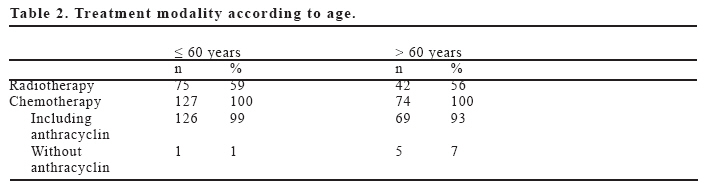
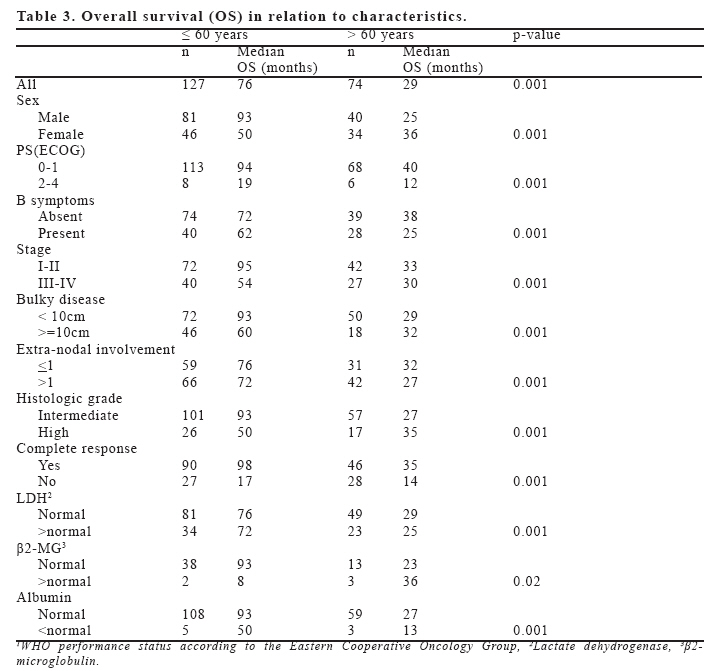
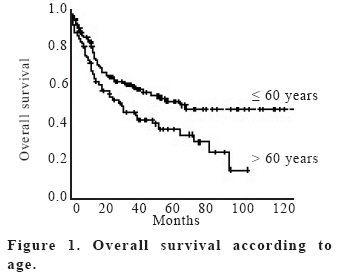
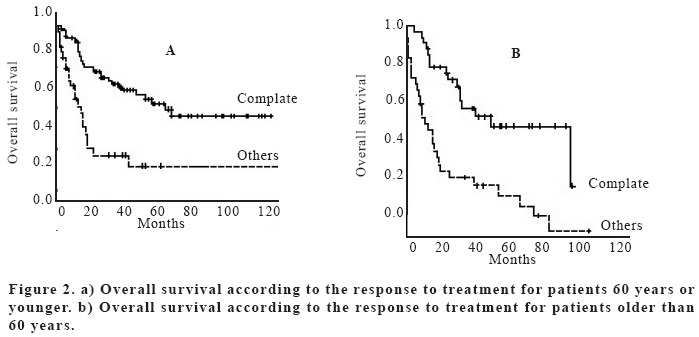
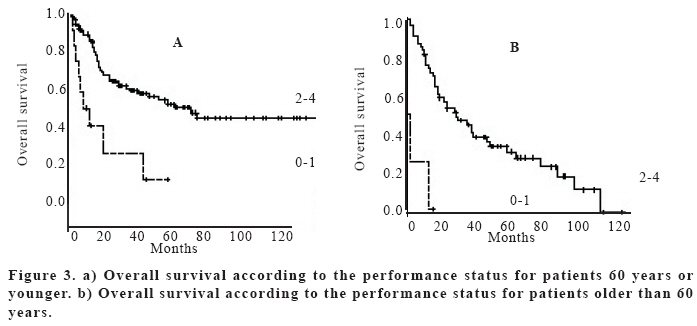
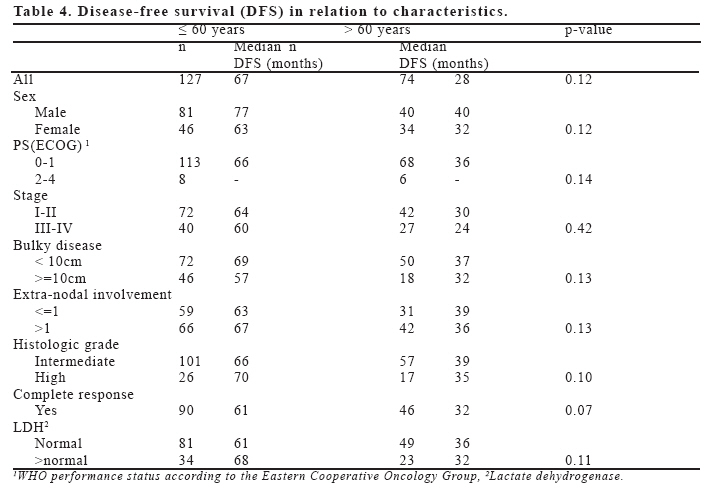
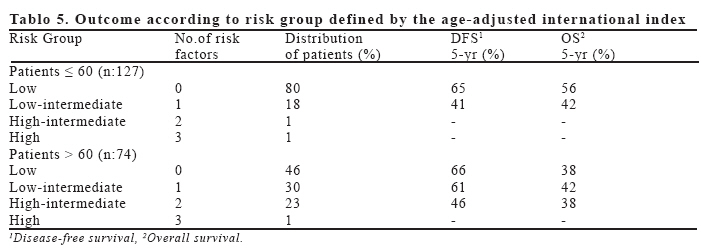
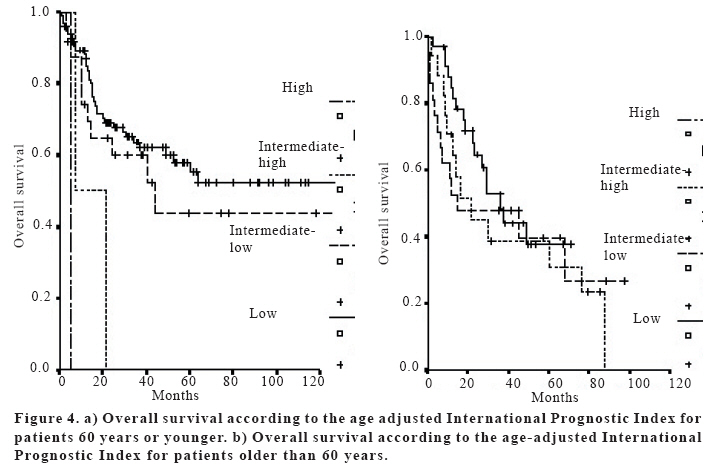
European Journal of General Medicine, Vol. 3, No. 3, 2006, pp. 93-101 EFFECT OF AGE ON CHARACTERISTICS AND CLINICAL BEHAVIOR OF ADULT AGRESSIVE NON-HODGKIN’S LYMPHOMA Suleyman Alıcı, Sevil E. Bavbek, Mert Başaran, Haluk Onat Istanbul University, Institute of Oncology, Istanbul, Turkey Correspondence: Dr. Süleyman Alıcı Yüzüncü Yıl Üniversitesi Tıp Fakültesi İç Hastalıkları AD 65200, Van, Turkey Tel: 905353080820, Fax: 904322155051 E-mail: suleymanalici@yahoo.com Code Number: gm06021 Aim: The importance of age as a prognostic factor in aggressive non-Hodgkin’s lymphoma (NHL) remains controversial. It is not clear whether age is an independent factor or reflecting the limited physiologic reserves of the patients. Key words: Age, elderly patients, non-Hodgkin’s lymphoma INTRODUCTION Although the incidence of non-Hodgkin’s lymphoma (NHL) is steadily increasing, particularly in elderly patients (1,2), few studies have described histologic and clinical characteristics of the elderly NHL patients. In some diseases, such as diffuse large cell NHL, it is known that older age is associated with a poor outcome, and that elderly patients frequently have more clinical features associated with a poor prognosis, such as poor performance status (PS), B symptoms, or concomitant disease (3,4). The importance of age as a prognostic factor in aggressive NHL remains controversial. The age may be an independent factor, or may reflect the limited physiologic reserves of the body, i.e. cardiac performance, bone marrow population and renal function. The study was aimed at assessing the influence of age on the clinical characteristics, response, and survival in NHL. MATERIAL AND METHODS Patients The clinical records and pathologic material of patients with intermediate- or high-grade NHL treated at the Institute of Oncology, Istanbul University during the 10-year period from 1989-1998 were retrospectively reviewed. The material included only patients above 15 years of age. All clinical records were collected for registration and analyses of data. On completion of data registration in June 1998, 334 patients with A-NHL were registered, with a median follow-up of 26 months (range 1-120 months). Of these, 33 patients were excluded from the study because of concomitant component of low-grade lymphoma (LG-NHL, n = 33). Of the 301 remaining cases, 100 had incomplete clinical or follow-up data and were not included in this analysis. Thus, 201 patients were included in the study. Adult patients were eligible for this study if they had a follicular large-cell, diffuse small-cleaved cell, diffuse mixed, diffuse large-cell, or large-cell immunoblastic NHL according to the Working Formulation (WF), and had been treated with a combination- chemotherapy regimen containing doxorubicin. The clinical features evaluated for potential prognostic importance according to age were sex, performance status (PS), B symptoms, stage, bulky disease, number of extra-nodal disease sites, histologic grade, complete response to treatment, serum lactate dehydrogenase (LDH), β2-microglobulin and albumin levels. The Ann Arbor stage of the tumor was designed as I,II,III, and IV. Performance status was assessed according to the Eastern Cooperative Oncology Group scale, in which indicated that the patient had no symptoms; 1, the patients had symptoms but was ambulatory; 2, the patients was bedridden less than half the day; 3, the patients was bedridden half the day or longer; 4, the patient was chronically bedridden and required assistance with the activities of daily living; 5. Performance status was classified as 0-1 or 2-4. B symptoms were defined as recurrent fever (temperature, >38.3C), night sweats, or the loss of more than 10 percent of body weight. The recorded sites of extra-nodal involvement included the bone marrow, gastrointestinal tract, liver, lung, central nervous system, and other sites; the number of extra-nodal disease sites were recorded as 0,1 or more than 1. The largest dimension of the largest site of bulky disease was measured and reported as being less than 10 cm or as 10 cm or more. The serum LDH level was expressed as the ratio of the measured value to the upper limit of the normal range reported in the laboratory. The age-adjusted International Prognostic Index as described for patients with aggressive lymphomas was used for the 5 year survival analysis (5). Treatment regimen The early stage patients were administered a combination-chemotherapy regimen containing doxorubicin at 3-week intervals, usually followed by radiotherapy (45Gy/25fr) with “involved field” technique. In advanced stage patients with bulky disease, a combination-chemotherapy regimen containing doxorubicin was followed by radiotherapy (45Gy) of the initial bulky tumor volume. Patients were evaluated before treatment with a complete medical history, physical examination, complete blood count, chemistry profile, chest radiograph, chest, abdomen, and pelvic computed tomography (CT), and bone marrow biopsy. Response criteria and survival All patients underwent repeated staging at evaluations during and after therapy. Evaluations included physical examinations, biochemistry, radiologic examinations, and possible bone-marrow biopsy. During the entire study period, response evaluation was carried out using CT scanning. Response criteria were assessed according to WHO recommendations (6). The overall survival (OS) period was defined as the period from the histologic diagnosis to the date of death or latest follow-up examination. The disease free survival (DFS) period was defined from the time of first CR to first relapse, last follow-up or death. Statistics Individual clinical features were analysed with chi-square test. Comparative statistics were done by univariate analysis of variance (SPSS). Survival analysis was carried out using the Kaplan-Meier method (7), and differences in survival rates were analysed using the log-rank test (8). Multivariate analysis was performed by Cox’s proportional hazards method (9) to identify subsets of independent prognostic factors for DFS and OS. Variables reaching statistical significance (p<=0.05) at the univariate level were included in the multivariate analysis. RESULTS Patient characteristics Characteristics of 201 patients with respect to age are given in Table 1. Seventy-four (37%) of the patients were above 60 years of age and 40 of these were male (54%). Among the elderly, the median age was 66 (range 61-87) years. At last follow-up for this report, 103 patients (51%) were alive, 40% in the elderly and 57% in the younger patients, respectively. Median follow-up in younger and older patients were 37.6 (range 1-120), and 20.8 (range 1-58) months, respectively. No significant differences in the distribution of the different prognostic factors [sex, performance status (WHO 0-1/2-4), B symptoms, bulky disease (<10cm />=10cm), extra-nodal involvement site (1/≥2), histologic grade (intermediate/high), complete response (yes/other), serum LDH levels (normal/high), serum β2-microglobulin levels (normal/high), and serum albumin levels] were observed among patients younger or older than 60 years, whereas significant difference in the distribution of the stage were observed between the groups. Older patients presented with more advanced disease than younger patients (p=0.01). Intermediate-grade histology was the most common among both groups. Treatment characteristics Table 2 shows the distribution of the treatment components of radiotherapy and chemotherapy for the two age groups. All of the patients were treated. Although the percentages of those receiving chemotherapy were almost the same in the two age groups, the elderly received far less anthracycline-based chemotherapy (93% vs 99%). Radiotherapy-alone was given to 3 (4%) elderly patients, and chemotherapy-alone to 31 (42%) elderly patients. Complete remission The complete response rate in all of the patients was 63% (n=126). The complete response rates among the two age groups were 70% and 62%, respectively (p=0.31). There were no significant differences in the complete response rates according to prognostic factors (sex, performance status, B symptoms, stage, bulky disease, extra-nodal involvement site, histologic grade, complete response, serum LDH, β2-microglobulin, and albumin levels) between the two age groups. Overall survival Table 3 summarizes the median overall survival (months) of the elderly and younger group. The median overall duration of survival for the 201 patients was 50 months. The Kaplan-Meier method estimated the five year survival at 47%. Median survival in younger and older patients were 75 months and 29 months, respectively (p=0.0001). Five years overall survival rates in younger and older patients were 52% and 40%, respectively (p=0.036) (Figure 1). There were significant differences in the median survival according to prognostic factors (sex, PS, B symptoms, stage, bulky disease, extra-nodal involvement site, histologic grade, complete response, serum LDH, β2-microglobulin, and albumin levels) between the two age groups in univariate analyses (p=0.001). In the multivariate analyses response to treatment (complete response and not complete response) (p=0.005) (Figure 2), and performance status (p=0.04) (Figure 3) retained significant as prognostic factors for overall survival. Disease-free survival The median disease-free survival (months) of the two age groups according to the prognostic factors are given in the Table 4. There was no significant difference in disease-free survival at five years between the two age groups (p=0.12). Age-adjusted prognostic index An age-adjusted prognostic index was determined for the elderly patients with intermediate and high-grade histology, using the variables of serum LDH, performance status, number of extra-nodal involvement sites, and stage. According to age-adjusted prognostic index risk groups in younger and older, 77%-45% of patients were in the low risk group; 18%-29% low-intermediate risk group, 1%-22 % intermediate-high risk group, and 1%-1% high risk group, respectively. According to age-adjusted prognostic index risk groups (5), five years overall survival rates in younger and older age groups were 56%-38%, 42%-42%, and 0%-38%, respectively (Table 5) (Figure 4). DISCUSSION The age limit above which the “elderly patient” is defined varies in most studies from 60 to 70 years. More than 50% of cancers occur above the age of 65 years (10,11,12), and 18%-38% of non-Hodgkin’s lymphoma is diagnosed in the elderly (10,11,13). In the current study 37% of the patients were above 60 years of age. Literature review suggests that 60 (14,15) and 65 years (16,17) are most commonly used as the discriminating ages in various studies, investigating prognostic importance of age in lymphomas. In accordance with the above-mentioned data, we chose 60 years in the present study as a cutoff point. When the characteristics of elderly patients group are compared with younger patients, only distribution of clinical stage is significantly different. Older patients presented with more advanced disease than younger patients. This difference is not easy to explain. Several points regarding treatment results of NHL patients in different age groups should be illuminated. The first is whether the responsiveness of aggressive NHL to chemotherapy depends on the patients age. Our data showed that the same CR rate was achieved whether the patient was older than 60 years or younger. The age of the patients did not influence the biological characteristic of chemosensivity of the aggressive NHL. Our data correspond to the results of Vose et al. (18) and Kovner et al. (19), who showed a similar CR rate in these age groups, but differ from the results of the Shipp et al. (5) and SWOG study (20), where the CR rate decreased with age. It may be concluded that the responsiveness of NHL in different age groups does not differ substantially. The achievement of a complete response is a clue for curing lymphoma. A more important end point is the survival benefit of the patients rather than the response rate itself. For patients above 60 years of age, the relapse rate was much higher and in addition to this, complete response rate was also tended to be lower than that of younger patients. These findings may account for the highly significant difference in median overall survival rate and tendency to lower disease-free survival rate for the older group. The survival of the patients in different age groups is the second point that should be addressed. Median survival of patients who had already succumbed to their disease was tended to be shorter in the age group than in the young (14 vs. 12 months) (but not significantly). On the other hand, median follow-up time of the groups was different (37.6 vs. 20.8 months). In our series, among eleven parameters tested (sex, PS, B symptoms, stage, bulky disease, extra-nodal involvement site, histologic grade, response to treatment, serum LDH, β2-microglobulin and albumin levels), these parameters appeared as the poor prognostic factors using univariate analysis. In the multivariate analysis, patients who lived for at least 5 years were characterized by complete response and good PS with the last two parameters having the same effect. Complete response is the most significant prognostic parameter in intermediate and high-grade NHL (21) and should be the goal of the treatment for such patients. In this series, survival was also influenced by performances status of the patients in addition to the response to treatment. The better the performance status, the better the complete response rate among old patients. The finding is in agreement with Domontet et al. (22), who found performance status to be among the independent prognostic factors of elderly NHL patients. This may also reflect the fact that the patients with poor initial performance status were treated with a reduced dose. Although, a decrease in immune surveillance has been suggested as a factor responsible for this poorer outcome, direct evidence of this defect as a contributory factor has not been demonstrated. Why older age has an adverse effect on patient outcome is not completely understood: a low survival rate and an increase in death rate may be due to the presence of poorer conditions in the elderly, mostly because of concomitant diseases (3,4). Our study shows that this poor outcome in the elderly patients may be related to a more aggressive disease: 24% of our patients had two or three adverse prognostic factors as described in the International Prognostic Index. In comparison with the age-adjusted IPI (age criterion 60 years) (5) the survival at five years for each index value was inferior in this study. Why elderly patients present a more aggressive lymphoma is not known. Usually, solid tumors in elderly patients are considered less aggressive and less proliferative than in young people. As lymphomas are tumors of the immune system, they may be associated with a more profound immune deficiency than solid tumors and a higher propency to grow and to disseminate. In conclusion, this study confirms the poor outcome observed in elderly patients with lymphoma. These elderly patients do not have specific histologic or clinical characteristics, nor they have more adverse prognostic features. However, the outcome of elderly and young patients is clearly related to the number of adverse prognostic factors, as shown in Table 5. Thus, age is not sufficient to discriminate patients with a poor outcome, but complete response and PS are necessary to define a subgroup of patients with very poor outcome. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06021t4.jpg] [gm06021f2.jpg] [gm06021f3.jpg] [gm06021f1.jpg] [gm06021t5.jpg] [gm06021f4.jpg] [gm06021t2.jpg] [gm06021t3.jpg] [gm06021t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}