 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
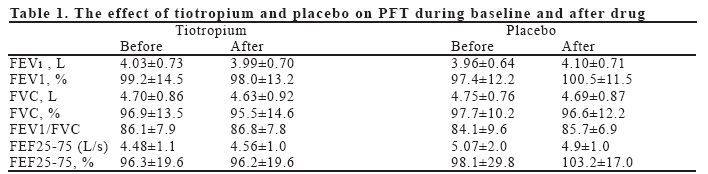
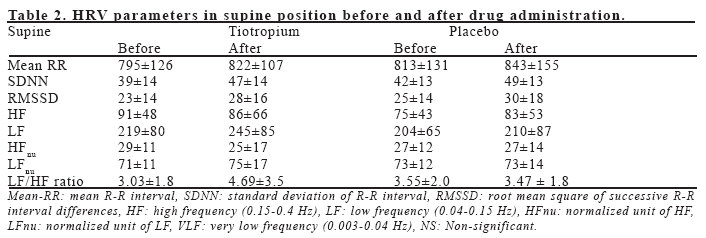
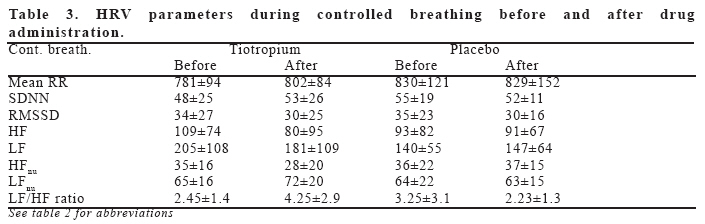
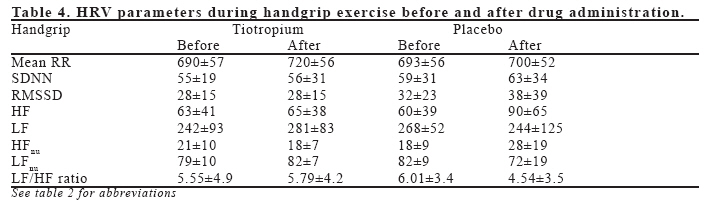
European Journal of General Medicine, Vol. 3, No. 3, 2006, pp. 102-107 SINGLE DOSE OF TIOTROPIUM DOES NOT EFFECT HEART RATE VARIABILITY Mehmet Unlu1, Mehmet Melek2, Fatma Fidan1, Celal Kilit2, Levent Tetik1, Dayimi Kaya3 Afyon Kocatepe University, School of Medicine, Departments of Chest Disease1 and Cardiology2, Afyon, 3Department of Cardiology, Ege Saglik Hospital, Izmir, Turkey Correspondence: Mehmet Unlu Address: Beyazit Mah. Gumuskent Sit. 119 Sk. C1 03200-Afyon, Turkey Tel:902722171753, Fax:2722172029 E-mail: munlu@aku.edu.tr Code Number: gm06022 Aim: Anticholinergic drugs may alter cardiac autonomic modulation. The aim of this study was to investigate the effects of inhaled tiotropium on heart rate variability (HRV). Key words: Tiotropium, heart rate variability, healthy volunteer INTRODUCTION Chronic obstructive pulmonary disease (COPD) is characterized by reduced expiratory airflow and the symptoms of cough, sputum production and dyspnea (1). The breathlessness associated with COPD develops over many years, is a major reason for seeking medical care and eventually limits daily activities (2). Bronchodilators are the mainstay of drug therapy for COPD given their ability to improve airflow and reduce breathlessness, the latter probably being related to reduced hyperinflation (3). Inhaled anticholinergic drugs such as ipratropium have been used since the 1970s in COPD and have emerged as a safe and effective therapy (1,4). A limitation of these agents is the need for frequent (i.e. four times daily) dosing. Tiotropium bromide is a member of the quaternary ammonium class of anticholinergic bronchodilators that dilate bronchial smooth muscle through antagonism of muscarinic receptors located in airway smooth muscle. Tiotropium bromide binds with similar affinity to muscarinic subtype M1, M2 and M3 receptors; however, the drug dissociates much more slowly from M1 and M3 receptors than from M2 receptors (5). Consequently, tiotropium bromide has a long duration of action allowing once daily administration in patients with COPD. Dry mouth was the most common event reported with tiotropium according to the combined results of the two 1-year placebo-controlled trials (6). There were no clinically significant changes in vital signs, 12-lead ECG or laboratory values during one year’s treatment with tiotropium (7). Heart rate variability (HRV), which is a non invasive diagnostic method, has been used to determine risk stratification in cardiological and noncardiological diseases. Abnormal cardiac autonomic function was identified with HRV in left ventricular dysfunction, diabetes mellitus and after myocardial infarction (8-14). The risk was estimated with frequency and time domain analyses of HRV in short term recordings (5 minutes). However, to date, the effects of tiotropium on HRV have not been studied. Different conditions such as upright position, exercise, and mental stress induce sympathetic stimulation and consequently change heart rate and HRV parameters (15,16). The aim of this study was to investigate the effects of tiotropium on cardiac autonomic function both at rest, during controlled breathing and mild exercise. MATERIAL AND METHODS Subjects Eleven healthy male volunteers, mean age 26±2 years (range 23 to 28 years), were studied in a randomized, double blind, placebo-controlled, crossover design study. The subjects with diabetes mellitus, coronary artery disease, respiratory, neurological or any other systemic disorder that might influence autonomic function, and those with a history of allergy to the drugs and smoking were excluded from the study. Their physical examinations and resting 12-lead electrocardiograms (ECG) were normal. Routine biochemical and hematological values including fasting blood glucose, blood urea nitrogen, serum electrolytes and hemoglobin levels were in normal ranges as well. The study was approved by the Joint Committee on Ethics of the Afyon Kocatepe University. Written informed consent was obtained from all participants before attending the study. All participants were asked to refrain from alcohol and caffeine-containing beverage and strenuous exercise for 24 hours prior to each study session. Study design All subjects underwent full physical examination and no abnormal findings was observed. They all had a light breakfast after an overnight period of fasting and taken to a quite, dimly lighted room with a temperature of 22-24°C. The studies were performed between 09:00 am and 12:00 am to avoid circadian variation of HRV parameters. Pulmonary function measurements (Forced vital capacity (FVC) forced expiratory volume in 1 second (FEV1), forced midexpiratory airflow 25–75 (FEF25–75)) were performed using a Dry Spirometer (Spirobank, MIR, Italy). All participants were taken to the test room and allowed to rest in supine position at least 15 minutes on a comfortable bed to stabilize heart rate. After this resting period, HRV parameters were calculated from the continuous ECG records performed at supine position for 5-minute, during controlled breathing for 5-minute and during handgrip exercise in sitting position for 5-minute intervals. Participants breathed 15 times per minute in respect of a metronome in controlled breathing period. They performed an isometric handgrip exercise at 25% of their predetermined maximum volunteer capacity in a manner of 45-second contraction and 15-second resting per minute using Jamar hydraulic hand dynamometer (Sammons Preston, Canada). Basal HRV data and pulmonary function tests were obtained before administration of drugs (pre-drug phase). The subjects were instructed, trained, and assessed on use of HandiHaler®. Subjects self-administered single dose placebo capsules including lactose or tiotropium capsules (18 μg) with the HandiHaler®. All subjects directly inhaled the drug after full expiration and then held their breath for 10 seconds. The order of administration of test drugs was randomized and subjects were blinded to the test drug received. The onset of action for tiotropium bromide is 43.5 minutes and mean plasma elimination half life is 5-6 days (17). With regard to this information, HRV data and pulmonary function tests were obtained once more, ninety minutes after drug administration (post-drug phase). Blood pressure measurements were obtained from left arm supported at heart level by trained physician using sphygmomanometer prior to and after each period. All participants attended two testing sessions separated by at least 10 days to eliminate the possibility of carryover effects from the previous test for each study drug. HRV analysis ECG data were fed to a personal computer and digitized via an analog-to-digital conversion board (PC-ECG 1200, Norav Medical Ltd, Israel). All records were visually examined and manually over-read to verify beat classification. Abnormal beats and areas of artifact were automatically and manually identified and excluded. HRV analysis was performed using Heart Rate Variability Software (version 4.2.0, Norav Medical Ltd, Israel). Both time and frequency domain analyses were performed. For the time domain, mean R-R interval (mean-RR), the standard deviation of R-R interval (SDNN) and the root mean square of successive R-R interval differences (RMSSD) were measured. For the frequency domain analysis power spectral analysis based on the Fast Fourier transformation algorithm was used. Three components of power spectrum were computed following bandwidths: high frequency (HF) (0.15-0.4 Hz), low frequency (LF) (0.04-0.15 Hz) and very low frequency (VLF) (0.003-0.04 Hz). The normalized unit LF [LFnu=LF/(LF+HF)], normalized unit HF [HFnu=HF/(LF+HF)] and LF/HF ratio were also calculated. Statistical analysis Data are presented as mean ± standard deviation. Non-parametric continuous variables were analyzed with “Wilcoxon Signed Rank” test. Statistical analysis was performed using SPSS for Windows 10.0 (SPSS Inc., Chicago, Illinois). A p value <0.05 was considered as statistically significant. RESULTS All participants tolerated the study well and no adverse side effects such as palpitation, tremor, headache and rhythm disturbance was observed. There were no statistically significant differences in pulmonary function parameters (Table 1) and in all baseline HRV parameters obtained before each drug administration (p >0.05). HRV parameters obtained after each drug administration were found not to be different during supine position, controlled breathing and handgrip exercise. The results of time and frequency domain parameters of HRV during supine position, controlled breathing and handgrip exercise before and after each drug administration are shown in Tables 2, 3, 4, respectively. DISCUSSION The main finding of the present study was that administration of single dose 18 μg tiotropium did not change HRV parameters during rest and autonomic maneuvers (controlled respiration and handgrip exercise) in healthy individuals. Bronchodilators are currently the mainstay of drug therapy for COPD (18). Anticholinergic and B2-adrenergic agents are widely used as a bronchodilator therapy in treatment of patients with respiratory system disorders. COPD is a disease state characterized by airflow limitation that is not fully reversible. Numerous studies have shown appreciable improvement in lung function with bronchodilator therapy in COPD patients, not specifically selected based on standard reversibility criteria (19). COPD appears to be more effectively treated by anticholinergic drugs than by sympathomimetics (18), probably due, in part, to the role of the cholinergic nervous system in controlling airway tone in these patients (20). In current treatment guidelines, anticholinergics are recommended for maintenance therapy in COPD (19,21). Vagally mediated bronchoconstriction is thought to be the major reversible component of airway obstruction in patients with COPD (17). In our study, single dose tiotropium is found not to alter pulmonary function tests in healthy subjects. This is considered to be related with lack of bronchoconstriction and vagal tonus increase in them. The ideal antimuscarinic for the treatment of asthma and COPD should inhibit airway bronchoconstriction by antagonizing M1 and M3, but not M2 muscarinic receptors. Tiotropium, a potent and long-lasting bronchodilator with kinetic selectivity for M1 and M3 receptors, is the most successful of the new antimuscarinic drugs. In clinical trials, tiotropium was effective and had advantages over the nonselective agent ipratroprium. The safety profile of quaternary antimuscarinic bronchodilators is superior to that of beta-agonists, particularly regarding cardiovascular side effects (22,23). The autonomic nervous system plays a major role in normal physiological function and in the pathogenesis of many medical disorders. Measurement of HRV provides an easily applied non-invasive method of assessing autonomic function. This has helped to clarify the role of the autonomic nervous system in regulating the cardiovascular response to maneuvers like controlled respiration (parasympathetic dominance) and exertion (sympathetic dominance) (24). Autonomic dysfunction plays an important role in the pathophysiology of cardiovascular diseases including ischemic heart disease, heart failure, diabetes mellitus and hypertension. Reduced parasympathetic activity in these patients have been found to be associated with malign ventricular arrhythmias and sudden cardiac death. Patients who have marked autonomic dysfunction leading to reduced HRV are at increased risk of premature death (8-14). Hypoxia in chronic respiratory disease can also induce autonomic abnormalities leading to reduced HRV (25). Systemic administrations of anticholinergic drugs have side effects on cardiovascular system like tachycardia, tremor, arrhythmias and alteration in blood pressure. However, the effect of the inhaled form of these drugs on cardiac autonomic function has not been well defined (26-28). In a study examining the effect of ipratropium on respiratory sinus arrhythmia, a non-specific indicator of parasympathetic modulation of heart rate, it has been shown to have no effect on asthmatic subjects (28). In our previous study we showed that inhalation of a single dose of ipratropium decreases parasympathetic modulation of heart rate in healthy men and this decrease in parasympathetic modulation of the heart occurs during mild exercise (29). In the current study, tiotropium is found not to affect autonomic tonus and modulation in healthy individuals during increased sympathetic and parasympathetic activity as it has no effect on time and frequency domain parameters of HRV by single dose administration during controlled breathing and light exercise. We think that the different effect of tiotropium on cardiac autonomic modulation may be due to high selectivity for M1 and M3 receptors compared to ipratropium. Study Limitations; the present study not only included a small number of healthy volunteers but also short-term records were obtained. Also they were all young males. But the people using tiotropium for treatment of COPD are older than our study group and they have comorbidities. Therefore, our results do not reflect the overall effects of these drug on cardiac autonomic function and the results may not be completely generalized to all patients with respiratory diseases. We administered only single dose of drug, so we could not consider about the long term effect of tiotropium. In conclusions, administration of single dose 18 μg tiotropium did not effect cardiac autonomic modulations in healthy volunteers. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06022t4.jpg] [gm06022t3.jpg] [gm06022t2.jpg] [gm06022t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}