 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
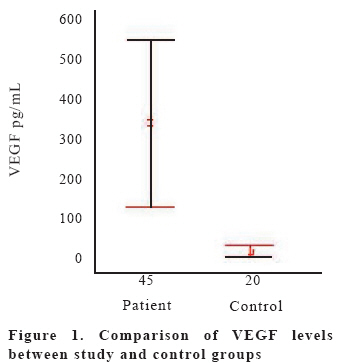
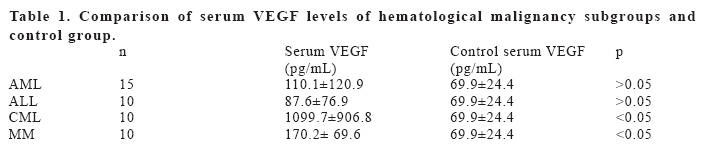
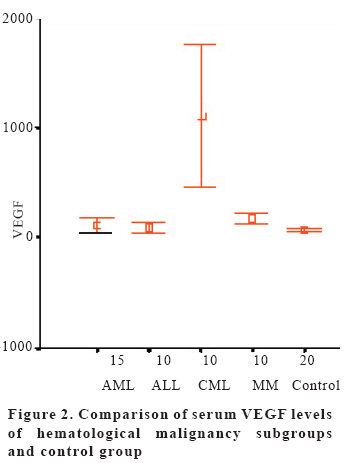
European Journal of General Medicine, Vol. 3, No. 3, 2006, pp. 116-120 SERUM VASCULAR ENDOTHELIAL GROWTH FACTOR LEVEL IN PATIENTS WITH HEMATOLOGICAL MALIGNANCIES Fuat Erdem1 , Mehmet Gündogdu1, Ahmet Kiziltunç2 Ataturk University, Faculty of Medicine, Division of Hematology of the Department of Internal Medicine1, Department of Biochemistry2, Erzurum, Turkey Correspondence: Fuat Erdem University of Ataturk, Medical School Internal Medicine, Division of Hematology 25240 Erzurum, Turkey Telephone: 904422361212-1539 E-mail: fuaterdem@yahoo.com Code Number: gm06024 Aim: Angiogenesis is an important factor in tumoral progression, metastasis and invasion. More recently, it has also been found to play a particular role in hematological malignancies. Key words:Serum Vascular Endothelial Growth Factor (VEGF), Hematological Malignancy INTRODUCTION Formation of new vascular structures is referred to as angiogenesis (1). Development of blood vessels depends on the balance between pro-angiogenic and anti-angiogenic factors. This process necessitates many physiological and pathological mechanisms. Angiogenesis has important roles in many physiological processes such as wound healing, embryological development and reproduction (2). It also has important roles in tumoral progression, metastasis and invasion. Recently, it has been shown that there is an increase in vascular density of bone marrow in patients harboring hematological malignancies (3, 4-6). Continuous supply of oxygen, growth factors and nutrients needed for progression, metastasis and invasion of the tumor tissue necessitates development of new vascular structures. Diffusion from surrounding tissues is the main support of tumors lacking new vascular structures. However, this method is no longer sufficient for adequate oxygenation of tumors growing from 100 μm to 200 μm. Beyond this critical volume, angiogenesis is required for progression and metastasis (7-10). Angiogenesis is a complex and dynamic processes mediated by many pro-angiogenic and anti-angiogenic molecules. Disruption of the balance between pro-angiogenic and anti-angiogenic factors in favor of pro-angiogenic factors leads to formation of new vascular structures. Tumor cells, fibroblasts, monocytes and degradation of collagen matrix are the main sources of angiogenic factors. Cytokines, VEGF and basic fibroblast growth factor (bFGF) are the most potent stimulators of angiogenesis (10-12). The aim of this study is to evaluate serum level of VEGF in patients with hematological malignancies. MATERIAL AND METHODS Between 2003 and 2004, 45 patients were followed up due to their documented hematological malignancies at the Hematology Division of the Department of Internal Medicine of Atatürk University Medical School. There were 25 (56%) male and 20 (44%) female patients. The mean age of the patients was 46±20 years. Of 45 patients who were followed up, 15 had AML, 10 ALL, 10 MM, and 10 CML. Mean age of the AML patients was 32.6±18.8 years and there were 10 male and 5 female patients in this group. There were 6 male and 4 female patients in ALL group and their mean age was 48.9±18.8 years. The mean age was 56.9±14.7 years in MM group (5 male, 5 female) and 56.3±16.7 in CML group (4 male, 6 female). Accordingly, twenty healthy volunteers were included in the study as the controls (12 male, 8 female; mean age 34.0±11.9 years). Serum samples taken from patients were stored at -80°C and serum VEGF levels were determined by Enzyme Linked Immune Assay (ELISA) method. VEGF study procedure: VEGF standard solution was diluted with 1 mL calibrator diluent. Serum samples taken from patients were also treated with the same diluent (1 mL). 1000, 500, 250, 125, 62.5, 31.2 and 15.6 pg/mL solutions were prepared from the standard solution. After adding 100 μL assay diluent to sample wells, 100μL of samples were added to the solution. On the other hand, only 100 μL of standard solution were added to standard wells. The plate was incubated at room temperature for two hours. All of the wells were washed with wash buffer three times. Plates were dried with blotting paper. After adding 200 μL of VEGF conjugate to each well, solutions were re-incubated at room temperature for another two hours. All of the wells were washed again with wash buffer three times. 200 μL of substrate solution were added to each well and incubated at room temperature for 25 minutes. After adding 50 μL of stop solution and mixing, absorbance at 450–540 nm reference wavelength was measured. Results were recorded according to standard curve as pg/ml. Statistical analysis was performed using commercially available SPSS 11.0 software. Data were expressed as mean±standard deviation. Comparison between groups was performed using the Mann-Whitney U-test. p<0.05 was considered statistically significant. RESULTS Mean serum VEGF level for the 45 patients with hematological malignancies was 338.4±587.6 pg/mL and 69.9±24.4 pg/mL for the control group. Serum VEGF levels of the patients with hematological malignancies were significantly higher than those of the control group (p<0.05) (Figure 1). Further subgroup analysis of hematological malignancy group (AML, ALL, MM, CML) revealed higher serum VEGF levels for each subgroup than the control group. However, only the CML subgroup and the MM subgroup demonstrated statistically significant difference compared to the control group (p<0.05). Nevertheless, serum VEGF levels of CML subgroup (1099.7±906.8 pg/mL) were also significantly different from the other subgroups (Table 1, Figure 2). Regarding serum VEGF levels, the difference between AML subgroup and ALL subgroup was not statistically significant (p>0.05). Serum VEGF level of CML subgroup (1099.7±906.8 pg/mL) was significantly different from that of the AML subgroup (110.1±120.9 pg/mL) (p<0.05) (Figure 3). Difference between the AML subgroup and the MM subgroup regarding serum VEGF levels was statistically significantly in favor of the MM subgroup (p<0.05). DISCUSSION Recently, the fact that angiogenesis may have an important role in hematological malignancies has attracted considerable attention and this has lead to conducting of new studies regarding the role of neovascularization in adult and pediatric acute leukemia, chronic leukemia, myelodysplastic syndromes, lymphomas and multiple myeloma (6,13-19). Although increased angiogenesis in solid hematological tumors such as lymphomas looks reasonable in the light of the pathogenesis underlying solid tumor-induced angiogenesis, it is difficult to answer the question why tumors like acute leukemia that are liquid in nature induce angiogenesis. Since bone marrow-infiltrating acute leukemia cells do not form a “mass” like solid tumors, the explanation of increased oxygen and nutrient consumption inducing angiogenesis is not sufficient for these tumors. However, many studies have demonstrated increased angiogenesis and angiogenic factors in acute leukemia (6,13-19). Recent studies have also demonstrated that angiogenic cytokines, particularly VEGF, have crucial roles in hematopoieses via signal conduction systems (20). Wierzbowska et al. (21) have found in their study in which 39 AML and 15 ALL patients were included, that there was no significant difference between the control and study groups regarding serum VEGF levels. However, they have demonstrated that serum VEGFR1 and VEGFR2 levels were significantly increased in both ALL and AML groups. Our findings demonstrating higher, but not statistically significant, serum VEGF levels of newly diagnosed 15 AML patients than the control group are concordant with Wierbowska et al’s study. Wierbowska et al. had also found increased serum VEGF levels compared to the control group in their study with 39 AML patients. It can be speculated that sVEGFR2 and particularly sVEGFR1 levels may be much more important than VEGF for AML patients. Aguayo et al. (22) have examined VEGF and bFGF levels with the ELISA technique and have found higher VEGF and bFGF levels in the study group than in the control group. They have also demonstrated the correlation between shorter survival and increased VEGF levels. According to these findings they concluded that plasma VEGF levels have prognostic value for AML patients. As also demonstrated in our study, another study including 23 CLL, 20 ALL, 24 CML, 30 AML and 32 MDS patients have demonstrated that CML patients have the highest serum VEGF levels and except ALL patients, all other groups had higher VEGF levels than the control group (13). Previous studies have shown that VEGF has a direct stimulatory effect on migration and proliferation of myeloma cells via paracrine and autocrine stimulation. VEGF has effects on many bone marrow cells including B cells and myeloid cells (20). Multiple myeloma is perhaps the most intensively studied disease for angiogenesis. Urba ska-Rys et al. (23) have studied serum VEGF, bFGF, HGF and TGF1 levels in a cohort of 162 MM patients, 5 Waldenstroma patients and 31 healthy controls. They have found a correlation between these afore-mentioned angiogenic cytokines and the stage and grade of the disease. They have documented a correlation between VEGF and beta-2-microglobulin and LDH; that bFGF has reached the highest serum levels in stage III MM and that these cytokines are found in higher levels than VEGF and bFGF in serum. Another study has also demonstrated that serum VEGF levels are higher in multiple myeloma compared to controls and there was a linear correlation between serum VEGF levels and the stage of the disease (24). Our study has also demonstrated statistically significant increase in serum VEGF levels for patients with hematological compared to controls. Previous studies have demonstrated the important roles of angiogenic cytokines in hematological malignancies similar to solid tumors. These studies will possibly improve the treatment protocols for hematological malignancies. In conclusion serum VEGF levels of the patients harboring hematological malignancies were found to be significantly higher than in the control group in our study. Particularly, the CML group was found to have the highest serum VEGF levels compared to the other patient groups and the controls. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06024t1.jpg] [gm06024f1.jpg] [gm06024f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}