 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
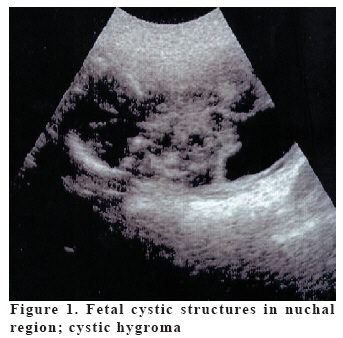
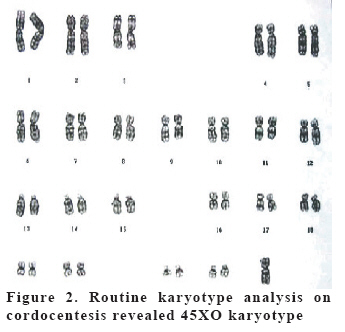
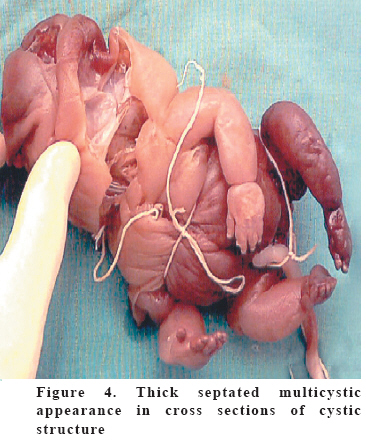
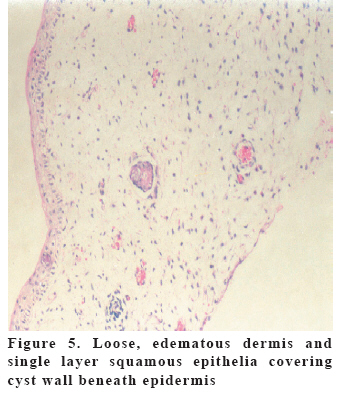
European Journal of General Medicine, Vol. 3, No. 3, 2006, pp. 136-138 TURNER SYNDROME AND CYSTIC HYGROMA Önder Şahin1, Ömer Doğru2, Nesrin Gürsan3, Mevlit İkbal4 Aynur Albayrak3, Cemal Gündoğdu3 Afyon Kocatepe University, Medical Faculty, Departments of Pathology1 and Pediatrics2, Afyon Atatürk University, Faculty of Medicine,Departments of Pathology3 and Genetics4, Erzurum Turkey Correspondence: Önder Şahin, MD Izmir istasyon cad. Mecidiye mah.Avcı apt, Kat:4 No:9 Afyon, Türkiye Tel: 902722142065, Fax: 902722142060 E-mail: kumtanesi34@yahoo.com Code Number: gm06028 Fetal cystic hygroma is characterized by single or multiple congenital cysts of the lymphatic system. Failure to establish venous drainage beginning around 40th day of gestation results in dilated disorganized lymph channels present as cystic hygromas. As a result lymphatic dilatation, lymphedema, single or multiloculated cystic hygromas are formed. A 30 year-old primigravid mother admitted for routine control of pregnancy and at ultrasonographic examination was found to have 90 mm diametered cystic lesion resembling cystic hygroma. Chromosomal analysis on cordosenthesis revealed 45XO karyotype. At 20th week of gestation pregnancy was terminated with parents’ consent. Here we presented the case to discuss cystic hygroma and Turner Syndrome association and autopsy findings of our case. Key words: Cystic hygroma, Turner Syndrome, nuchal region, antenatal ultrasonography INTRODUCTION Fetal nuchal cystic hygromas (NCH) are congenital malformations of the lymphatic system and can be defined as an area of sonolucency in the soft tissue of the occipital region, consisting of two symmetrical cavities completely separated by a midline septum (nuchal ligament), with or without internal trabeculae (multiloculated cysts). Diagnosis can be made at first trimester of pregnancy using vaginal ultrasonography (1). Cystic hygromas may subsequently disappear, thus emphasizing the importance of an early ultrasonographic examination. The association with chromosomal abnormalities has been reported in many studies (2-9) and therefore, fetal karyotype evaluation must be routinely carried out in these cases. The most common chromosomal abnormality associated with cystic hygroma is 45 XO (in 60% of all patients). Trisomy 13, 18, 21 and 47XXY are among other common chromosomal abnormalities(4-8). It is very difficult to determine the prognosis of a fetus with cystic hygroma since it may occur as an isolated finding or may be associated with chromosomal abnormalities (4), Mendelian disease, or other malformations. Its natural history is also variable. Ultrasonographic examination and karyotype analysis is essential for definite diagnosis and decision for termination of pregnancy. CASE A 30 year-old primigravid mother admitted for routine control of pregnancy was found to have 90 mm diametered cystic lesion resembling cystic hygroma at USG examination (Figure 1). Family history revealed no specific disease or congenital malformation. Blood sampling for karyotype study was done during cordocentesis. Routine karyotype analysis revealed 45XO (Figure 2). At 20th week of gestation pregnancy was terminated with parents’ consent. At autopsy fetus had fetal hydrops and was 450 g at weight. Crown-rump distance was 15 cm, crown-heel distance was 22 cm. Low onset hair line and short neck was present. Bright dark gray colored and 11x7x5 cm sized web like mass was surrounding the whole neck (Figure 3). Ecchymoses were extending from above umbilicus to distal lower extremities. Whole scalp was ecchymotic, the root of nose was flattened and micrognatia was present. Both ears were low onset, at level of mandibula. At left iliac area 1,5x1x0,5 cm sized mass was observed. Lymphedema on foot and hands was present. Nails were hypoplastic. Areolae were separate and unapparent. External genitalia was compatible with female genitalia. The length of umbilical cord was 24 cm and the diameter was 1 cm in thickest portion. The placental material was 70 g in weight and 15x7x5 cm in size. Serial cross sections at web forming tissue at cervical region revealed serous-hemorrhagic fluid containing cystic structure (Figure 4). At microscopic examination immature skin tissue covering cyst wall was seen (Figure 5). On autopsy, there was no cardiac, renal or any other malformation. Chromosomal analysis in cell culture of amniotic fluid revealed 45X0 karyotype. Whole scalp was ecchymotic, the root of nose was flattened and micrognatia was present. Both ears were low onset, at level of mandibula. At left iliac area 1,5x1x0,5 cm sized mass was observed. Lymphedema on foot and hands was present. Nails were hypoplastic. Areolae were separate and unapparent. External genitalia was compatible with female genitalia. The length of umbilical cord was 24 cm and the diameter was 1 cm in the thickest portion. The placental material was 70 g in weight and 15x7x5 cm in size. Serial cross sections at web forming tissue at cervical region revealed serous-hemorrhagic fluid containing cystic structure (Figure 4). At microscopic examination immature skin tissue covering cyst wall was seen (Figure 5). On autopsy, there was no cardiac, renal or any other malformation. Chromosomal analysis in cell culture of amniotic fluid revealed 45X0 karyotype. DISCUSSION Cystic hygroma is characterized by multiple congenital cysts generally located in cervical soft tissue and appears to be as a result of incordinance between internal jugular vein and jugular lymphatics (2,3). The frequency is about 0.1-0.5 percent. The frequency of accompanying organ anomalies is about 60-80% and karyotype anomalies 60-80%. Broad multilocular lesions, aneuploidi, fetal hydrops also may be present (4,6). Prenatal diagnosis is important in clinical approach. In early pregnancy especially transvaginal USG has a great role in detection of major or minor anomalies (7,10). Fetal karyotyping is an important diagnostic technique for cystic hygroma (5,9). Turner Syndrome, Trisomy 21, Trisomy and Trisomy 13 lie abnormal karyotypes may accompany to nuchal cystic hygroma. Bornstein et al have reported that chromosomal abnormalities were more frequent among patients with septated cystic hygroma compared with non-septated. Similarly we detected different sized multiple thick walled cysts at autopsy cross-sections. It is proposed that ultrasonographic detection of non septated cysts in second trimester presumes good prognosis (11). Cystic hygroma, a rare congenital development defect and accompanying chromosome anomaly monozomy 45X0 (Turner Syndrome) has been presented in order to remind the association between cystic hygroma and Turner Syndrome and emphasize the importance of prenatal diagnosis. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06028f4.jpg] [gm06028f2.jpg] [gm06028f3.jpg] [gm06028f1.jpg] [gm06028f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}