 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
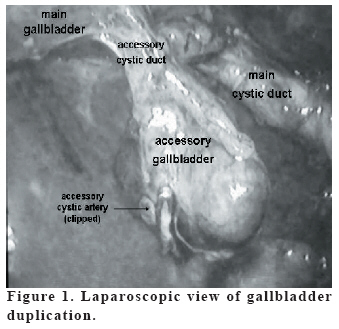
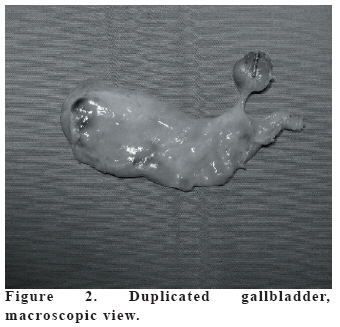
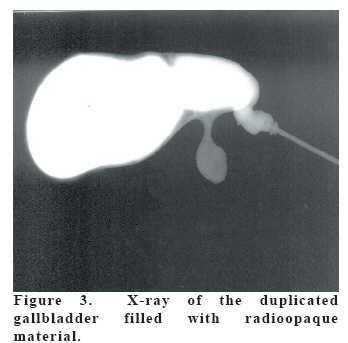
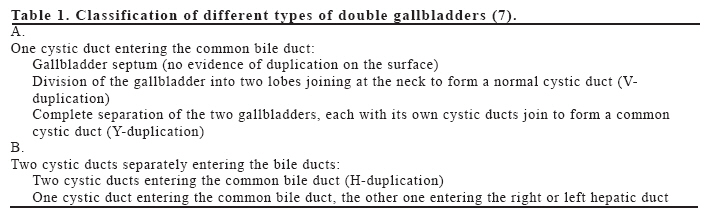
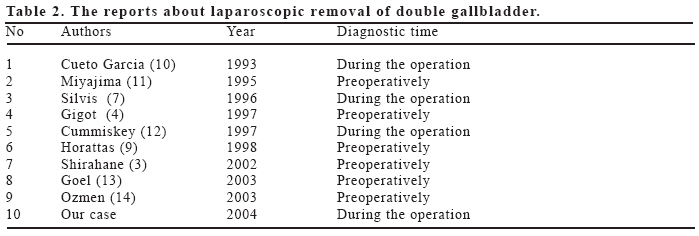
European Journal of General Medicine, Vol. 3, No. 3, 2006, pp. 142-145 GALLBLADDER DUPLICATION diagnosed and treated by laparoscopy İbrahim Barut, Ömer Rıdvan Tarhan, Uğur Doğru, Mahmut Bülbül Süleyman Demirel University Medical School, Department of General Surgery, Isparta, Turkey. Correspondence: Yrd. Doc. Dr. Ibrahim BARUT SDU Tıp Fakultesi Genel Cerrahi Anabilim Dalı, 32900 – Isparta, Türkiye Tel: 905324217997, Fax: 902462234284 E-mail: ibarutt@hotmail.com Code Number: gm06030 Gallbladder duplication is a rare congenital anomaly which is important in clinical practice because it may cause some clinical, surgical, and diagnostic problems. We present a case of duplicated gallbladder diagnosed and treated during laparoscopy. There was no sign in preoperative workup about the duplication. Ultrasonography revealed multiple stones in gallbladder and laparoscopic cholecystectomy was planned. Gallbladder duplication was detected during the operation and successfully treated by laparoscopy. This case illustrates the need for complete removal of both gallbladders during initial surgery. Precise intraoperative recognition of vascular and biliary anatomy-including abnormalities-is necessary to avoid mistakes during surgery. Key words: Gallbladder duplication, laparoscopic treatment INTRODUCTION Duplication of the gallbladder has been reported as an extremely rare congenital anomaly with an incidence of 1 in 3800-4000 autopsies (1-8). Laparoscopic Cholecystectomy (LC) has become a standard operation for the great majority of benign gallbladder diseases including congenital anomalies of the biliary tree and the gallbladder. However, a higher incidence of bile duct injury during LC has been reported in cases of a severely inflamed gallbladder or complex biliary anatomy (3). We report a case with double gallbladder that underwent successful LC. CASE A 55-year-old woman was admitted to our hospital with a right upper quadrant pain recurring for past 10 years. The pain was referring to her right shoulder after the meals. Physical examination showed Murphy’s sign on the right upper quadrant. Her blood values were within normal range. Plain abdominal radiography was normal. Ultrasound (US) of upper abdomen showed the gallbladder which is full of multiple calculi. US findings did not allow the differentiation of duplication because of the multiple stones and cystic ducts which were not identified. LC was planned and single dose antibiotic prophylaxis was performed with 1 g. Ceftazidim (Fortum®, Glaxo Smith Kline, Izmit, Turkey) an hour before the operation. Standard anesthetic procedure was performed to the patient. Nasogastric decompression was performed perioperatively and was removed at the completion of the procedure. At exploration, it’s surprised that there was a smaller accessory gallbladder and it was located anteriorly to the main one (Figure 1). The accessory cystic artery was isolated after careful dissection of Calot’s triangle and clips were placed on it. Two cystic ducts (main and accessory cystic ducts) were detected. The duct of accessory gallbladder joined with the main cystic duct in Y-shaped. After division of the cystic duct and arteries, the gallbladders were retracted cephalically, and the peritoneum is incised and the duplicated gallbladders are dissected from the liver. LC was successfully completed without any complication (Figure 2). No drain was used in the patient. The duration of the operation was 50 minutes. The postoperative period was uneventful, and the patient was discharged on the 2nd postoperative day. She was free of symptoms 12 months later. After the operation, the biliary stones were removed. The cystic duct catheterized and radioopaque material was given in order to demonstrate the gallbladder duplication in the surgical specimen (Figure 3). We couldn’t find any stone in accessory gallbladder. DISCUSSION Double gallbladders have been reported extremely rare. They may share a common cystic duct and be completely separated, or they may be divided by a septum. When they do not share a common outlet, the cystic ducts of double gallbladders open separately into the common bile duct or, less commonly, into the right hepatic duct (1, 4). According the Boyden classification (4), these congenital anomalies of gallbladder classified according to the ductal formation as bilobed (or bifid), “Y-shaped” and “H-shaped” (or ductular) gallbladder types. Classification of different types of double gallbladders is shown in table 1 (7). The gallbladder type of our case was compatible with the Y-shaped one. To date US, oral cholecystography, oral cholecysto-computed tomography, scintigraphy, magnetic resonance cholangiography, percutan transhepatic cholangiography and endoscopic retrograde cholangiopancreatography have been used preoperatively to diagnose gallbladder duplication (3-8). The differential diagnosis of gallbladder duplication from some gallbladder diseases is often difficult. They include choledochal cyst, gallbladder diverticulum, pericholecystic fluid collection, focal adenomyomatosis, a Phrygian cap, extrinsic fibrous bands across the gallbladder, and a folded gallbladder. And the diagnosis of double gallbladder is made preoperatively in fewer than half of cases. It is often found incidentally during the surgery for cholelithiasis (3, 5, 9). We also found the duplicated gallbladder during the LC for cholelithiasis. Main gallbladder was full of stones. Double gallbladder could not be demonstarted preoperatively by radiology probably due to this reason. Nevertheless, it can be diagnosed and treated by laparoscopy. Laparoscopic removal of duplicated gallbladder was reported before nine times. These cases were diagnosed preoperatively or detected incidentally at the time of surgery (Table 2). To our knowledge, the present case is the fourth patient diagnosed and treated during the LC (Table-2) (3, 4, 7, 9-14). We thought if gallbladder duplication was suspected at operation a cholangiogram could be attempted. And if there is no suspicion about the anatomy it’s unnecessary to be converted to open operation. Consequently, identification and definition of biliary anatomy is mandatory to prevent biliary system injury. Injury to the ductal system usually occurs during the dissection at the triangle of Calot, exposing the cystic duct. Cullen (15) emphasizes that meticulous dissection must be done, and the infundibulum of gallbladder must be retracted laterally to fully expose the cystic duct in order to avoid bile duct injury. All connective tissue and fat must be removed completely to clearly expose the junction of the cystic duct with the gallbladder, and cystic duct remnant must be leaved longer. Excessive use of electrocautery must be avoided during the dissection of cystic duct in the triangle of Calot, which may lead to stricture (13). In our case, we also performed very careful dissection for identification and definition of biliary anatomy during LC to prevent biliary system injury and double gallbladder with cholelithiasis was successfully removed. In conclusion, this case illustrates the need for complete removal of both gallbladders during initial surgery. Precise intraoperative recognition of vascular and biliary anatomy-including abnormalities is necessary to avoid mistakes during surgery. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06030f2.jpg] [gm06030f1.jpg] [gm06030t2.jpg] [gm06030f3.jpg] [gm06030t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}