 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 3, No. 4, 2006, pp. 152-158 EFFECTIVE VARIATIONS ON ACUTE MYOCARDIAL INFARCTION IN THE ELDERLY IN A CITY IN WEST OF TURKEY Alaettin Ünsal1, Ünal Ayrancı2, A.Alper Çevik3, Selma Metintaş1 Osmangazi University Medical School, Departments of Public Health1 and
Emergency Medicine3, Medico Social Center2, Eskisehir,
Turkey Code Number: gm06033 Abstract Aim: Although Turkey has one of the youngest populations when
compared with those of European and Middle Eastern countries, the proportion
of our elderly population has increased year-by-year and as has myocardial
illnesses in parallel. The aim was to investigate the effects of the monthly,
outdoor temperature and weekday variables on acute Myocardial Infarction (aMI)
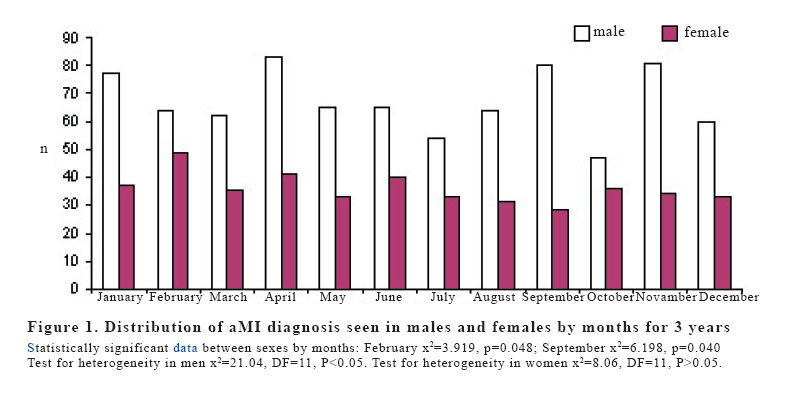
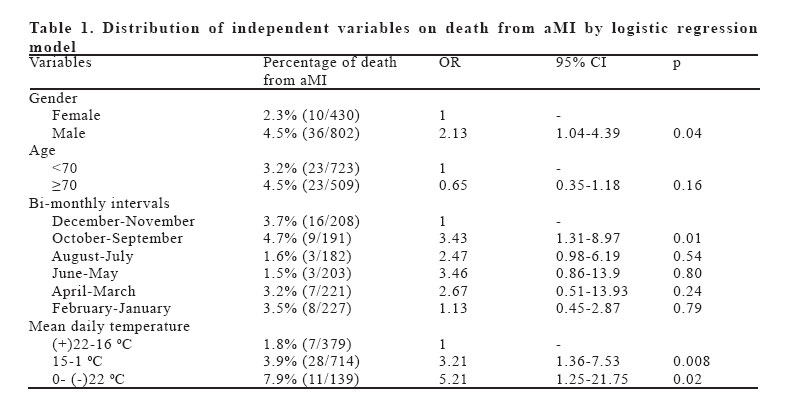
in the elderly, attending Emergency Departments (EDs). Key words: Climate, emergency, acute myocardial infarction, elderly INTRODUCTION World Health Organization (WHO) estimates that there will be a billion people over 60 years of age in the year 2020, and more than 70% of these will be in developing countries (1). Turkey has one of the youngest populations when compared with those of European and Middle Eastern countries. However, the proportion of our elderly population in total has increased year-by-year, with a 5.2% and 5.57% in 1995 and 2000 respectively (2). The leading cause of death in the elderly is cardiovascular disease, especially in developed countries. More than half of deaths from cardiovascular disease are due to acute myocardial infarction (aMI) (3-5). Although aMI is thought of as a middle-aged man's disease, 60% of aMI is seen in those over 65 years of age, and approximately 30% is seen in patients 75 years of age and older (6). Death and serious complications from aMI have a direct correlation with aging (7,8). More than 80% of aMI deaths are in those aged 65 and older, and 60% of aMI deaths are in those 75 years of age and older (9,10). Although the relationship between cardiovascular disease processes and environmental factors is not well identified, some studies have shown increased deaths from aMI related to the winter season (11-17). However, no relationship between outdoor temperature and aMI has been demonstrated (12,18). There is only limited data about the effects of temperature variations on aMI in the elderly, particularly in our country. The study was undertaken to look for additional data that might support or refute the hypothesis that temperature, monthly, and weekday variations affect the prevalence of AMI, and mortality from AMI. The way to definitively answer this question would have been to look in a large registry containing all cases of aMI, such as in our study. Thus, the aim of this study was to investigate the association for the elderly between myocardial infarction and environmental factors such as seasonal and temperature variations on fatal aMIs in EDs. MATERIAL AND METHODS Climatic characteristics in Eskisehir Eskisehir is under the effect of terrestrial climate in terms of its geography. The winter months are snowy, rainy and cold; the spring and autumn months are mild, cold and showery, while the summer months are sunny and hot. Mean yearly temperature is 11.1 0C, with large temperature variations ranging from -1 to +22 0C between months. Study population, data collection and procedure The entire patient records of all the secondary and tertiary healthcare hospitals'EDs located in the city of Eskisehir, North West of Turkey were retrospectively scanned in this study. These hospitals were comprised of the Hospital of Osmangazi University, the State Hospital, and the Hospital of the Social Insurance Association (SIA), having over 95% of the ED density in the city. The other two hospitals controlled by the State and SIA hospitals were excluded from the study since they are specific maternal hospitals. In total, 608,528 general patients had visited the EDs of these three health institutions during the three-year-period, 79,123 (13.0%) of which had been made by elder patients. aMI was diagnosed in 1.56% (1,232/79,123) of the total elderly visits to EDs. In this study, all recorded ED patients aged 60 and older as well as those having received a diagnosis of aMI in the EDs of three major hospitals between the dates of January 1st, 1998 and December 31st, 2000 were included in the study. All the illnesses of the patients presenting to the EDs had been classified according to the International Statistical Classification of Diseases-10 (ICD-10) classification (19). Of all the patient records, those diagnosed with aMI were determined through scanning. All of the demographic characteristics of those diagnosed with aMI were recorded on a questionnaire. The questionnaire, designed by the researchers, was compromised of information related to the demographic characteristics of the elderly, such as age, gender, main diseases at admittance, and disposition decisions (attendance to the hospital, ED treatment and discharge, death in the ED, and death at attendance to the ED), deaths due to aMI, and the presenting date to the EDs (day/month/year) according to data registered on the protocol register (a kind of notebook approved by the health authority to register the characteristics of patients). A patient with aMI attending to an ED was diagnosed by the following criteria: The existing symptoms consistent with aMI: elevated serum levels of cardiac enzymes, electrocardiography (ECG) findings coherent with aMI, and an interpretation and diagnosis by a cardiologist. Daily mean temperatures received from the mean values of the daily measures were taken from the Regional Weather and Meteorology Center located in the city of Eskisehir. Statistical Analysis Subtotals of the numbers of cases with aMI were calculated at monthly intervals for the 3-year-period. The total number of the cases occurring in each month, as well as for each day of the week, were calculated along with 95% confidence intervals (CIs) derived from the Poisson distribution, and a test for heterogeneity was applied. Statistical analyses were performed using general linear modeling and variance analysis (ANOVA) to analyze the mean of the adjusted number of aMI cases. Factors in the model included months and days of the week. These analyses were performed separately for women and men. The F test from ANOVA determined the overall main effect of the season. If the finding was significant (p<0.05), then the least significant difference test was used for post-hoc comparison of multiple means to determine which month and day of week were different. Coefficient correlation was calculated between the number of aMI cases and the daily temperature during the three years. Variations in frequency distributions within the study period were evaluated by Pearson Chi-Square. The importance of potential risk factors for mortality from AMI in EDs was assessed by adjusting logistic regression models. The model contained gender (female, male), age (60-69, ≥70), monthly intervals (January-February, March-April, May-June, July-August, September-October, November-December), and mean daily temperatures ((-)22-0, (+)1-15, (+)16-22 in oC)) as was advised by the Regional Weather and Meteorology Center, in addition to days of week (Monday, the other days). For each categorical variable the reference groups (female, <70 age of years, December-November, 22-16 0C, Monday) were selected and ORs were found. Written ethical approval The local authorities, those of the Osmangazi University School of Medicine, and the head doctors of the hospitals in Eskisehir, approved this study. RESULTS aMI was diagnosed in 1.56% (1,232/79,123) of the total elderly visits to EDs, namely 332 (1.47%) for the year 1998, 425 (1.53%) for 1999 and 475 (1.66%) for 2000. Of total aMI diagnosis, 802 (65.1%) were for men, and 430 (34.9%) for women, the difference was significant (p<0.001). The average age of the 1,232 aMI patients was 68.96±7.12 years, (range: 60-96 years). Although the average age of aMI in the female group (69.2±5.8 (min:62-max:96) was slightly higher than that of the other group (68.9±5.6 (min:60-max:94), it revealed no significant difference (p>0.05). The proportion of aMI cases in the age group 60-69 was higher than that in the age group of 70 and over (723 (58.7%) and 509 (41.3%), respectively) (p<0.001). Distribution of aMI diagnosis seen in males and females by months for the 3 years is presented in Figure 1. The months where aMI cases were the most frequently seen were April and November. When investigated whether aMI diagnosis changed according to months, it was seen that aMI diagnoses in males were significantly higher than females in the months of April and November (p<0.05) while higher in females than in males in the months of February and April (p>0.05). In general, there was no difference between men and women by months (x2=13.11, DF=11, P=0.29). When men and women were compared by months in aMI diagmosis, it was seen that in February aMI diagnosis in women was higher than that of men (p<0.05), however, in September aMI diagnosis in men was higher than that in women (p<0.05). In our study, the mean temperature of the city during the 3-year-period was 10.96±8.67 oC (from 22.60 oC to 29.60 oC). There was a prominent increase (8.1 oC) and decrease (5.4 oC) in mean temperatures in April and November, respectively. There was no correlation between the mean daily temperature and the number of aMI cases by linear regression analysis (R2=1%, F=0.867, p=0.352). The relationship between the mean numbers of aMI cases and the days of the week by gender did not reveal any difference (Test for heterogeneity for males, x2=9.43, DF=6, p>0.05; trends computed by variance analysis F=1.373, p=0.222 and the test for heterogeneity for females, x2 = 8.626, df=6, p>0.05, trends computed by variance analysis, F=1.301, p>0.05). The mean number of aMI cases on Mondays was higher than other weekdays for males (t=2.08, p<0.05) (Unshown data). The logistic regression model of the effects of the independent variables to predict death from aMI is shown in Table 1. In our study, it was found that the number of aMI cases who died in the EDs was 3.7% (46/1232). The independent variables found to have significant effects according to the logistic regression model, performed to identify indicators of death from aMI, were as follows: gender (male), two months intervals (October-September), and mean daily temperature (15-1 oC and 0-(-)22 oC). The proportion of death from aMI was 2.13 times higher in males than in females (p<0.05); 3.43 times higher in the months of September-October than in the months of November-December (p<0.05), and 5.21 and 3.21 times higher at temperatures of 15-1 oC and 0-(-) 22 oC, respectively (p<0.05, each one). DISCUSSION This small multicenter study describes the pattern of ED use by the elderly in three Turkish hospitals in the same city. In this study, the proportion of aMI cases was found to be significantly more in males than in females (65.1% and 34.9%, respectively). This finding was consistent with previous study results showing that aMI diagnosis was seen more in males than in females (13,20). Krgovic et al (1999) found that, in common with our study, myocardial infarctions in 1192 patients were seen at a proportion of 61.9% in male patients and at 38.1% in female patients (20). In previously conducted studies (21,22), although it was found that death rates from aMI in the aged did increase with age, in our study, no increase was found after the age of 70 when compared to age <70. One explanation for this could be that this study did not have as high a number of deaths from aMI deaths as those in other studies. In the current study, there was no relationship between aMI and the months (p>0.05) for females, whereas in contrast April and November revealed the highest numbers of aMI cases in men (p<0.05). As with the case in men, April and November demonstrated the highest numbers of aMI cases by sex (p>0.05). These months also had large increase and decrease trends in temperature, suggesting that temperature variations could play an important role in provoking aMI. In some studies, although the months of January and March had the highest number of aMI cases, no other differences were revealed between aMI and months (18,23,24). This study shows that male patients are at a higher risk compared to females. In this study, there was no correlation between the mean daily temperature and the number of aMI cases by linear regression analysis (R2=1%, F=0.867, p=0.352). This is consistent with another study (25) where weather conditions had been reported as not being a triggering factor for aMI. However, Thakur et al. showed that aMI cases did increase if temperatures were 16 oC or less (26). Although lower temperatures did show with a corresponding increase in the number of aMI cases in our study, further study is necessary to prove any association between temperature and aMI. The proportion of death from aMI in this study was 3.21 and 5.21 times higher at temperatures of 15-1 oC and 0-(-)22oC, respectively (p<0.05, each one), indicating that fatal aMI cases increase as mean daily temperature decreases. This finding is in line with other studies showing a linear increasing correlation between death from aMI and lower temperatures (27,28). This particularly demonstrates that in cold weather, patients with aMI and emergency services personnel should be vigilant. There is a lot of literature available on the weekly distribution of cardiac events: with some researchers finding an increased risk on Mondays for aMI cases (18,27). Some authors reported that aMI cases in the beginning of the week were higher (15); whereas others indicated aMI cases peaked on other days of week, or that there was no significant weekly variation at all (29). In addition, Sunday was reported to have the lowest rate of aMI (16,24,30). In our study, there were no significant differences between weekdays and the number of aMI presentations in the overall group and in females. However, Monday had the highest frequency of aMI presentations in males. These results may be related to variations of stress levels on workdays, which tend to be weekdays, as reported in the literature (18). Another important descriptor is the seasonal effect on aMI. In our study, the months where aMI cases were the most frequently seen were April and November (10.1% and 9.4%, respectively), followed by the months of January and February (9.3% and 9.2%, respectively) (p>0.05). In some studies related to the seasonal effect on aMI, it was found that aMI was more likely to occur in winter and spring than in other seasons of the year (31). Whether factors such as geographic latitude influence the pattern will always be questionable and the cause of the seasonal pattern of aMI cases is unclear (15,32,33). Several theories have been proposed to explain an increased prevalence of aMI cases in winter (15): Cold weather or a sudden change in the climate can increase arterial blood pressure (32,33), arterial spasm, platelet and red blood cell counts, blood viscosity (35), plasma fibrinogen, factor VII (33), and serum cholesterol levels (36). Concurrent infections during the winter months, particularly those involving the respiratory tract, have also been postulated as a trigger for acute cardiovascular events. Considering these findings and theories, further research is needed on the effect of seasons on aMI. In conclusion, our data suggests that not only the winter season or a cold environment; but also a rapid increase or decrease in daily temperature can also trigger acute coronary events, meriting further study. Independent predictors that we have identified in this study should be evaluated with a prospective series, which captures all cases of aMI, including those presenting as sudden death or with atypical or no symptoms. As the expected number of elderly in the community grows, we will also continue to see growth in the number of elderly patients in the ED. These larger numbers will place greater demands on ED staff since they require more time for placement in ED examination areas, attention to safety, and time and effort in the communication of the details of ED evaluation, management, and discharge instructions. Acknowledgments We thank all the head doctors and emergency service chiefs of the hospitals who helped in reaching the data REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06033f1.jpg] [gm06033t1.jpg] |
| |||||||||

{kind=link}
{kind=link}