 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 3, No. 4, 2006, pp. 159-166 EVALUATION OF ASTHMA CLINICS IN PRIMARY CARE IN KUWAIT Badria M.Al-Kanderi1, Fatma A. Al-Muhaileej2, Tahani Al-Khalaf3 South Sabah Salem Clinic, Hawalli1, Hadiya Clinic, Ahmadi2,
Dasma Clinic, Capital3, Kuwait Code Number: st06034 Abstract Aim: To determine the difference between asthmatics followed in asthma
clinics , and asthmatics followed in non-asthma clinics in terms of knowledge
about asthma definition, knowledge about provokers, proper inhaler technique,
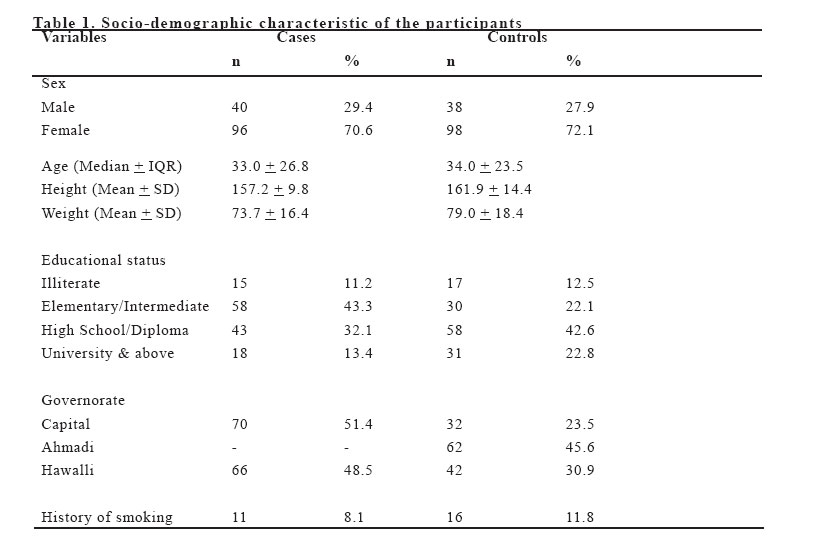
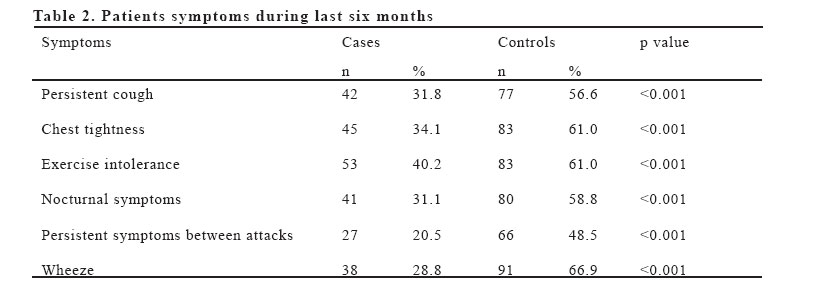
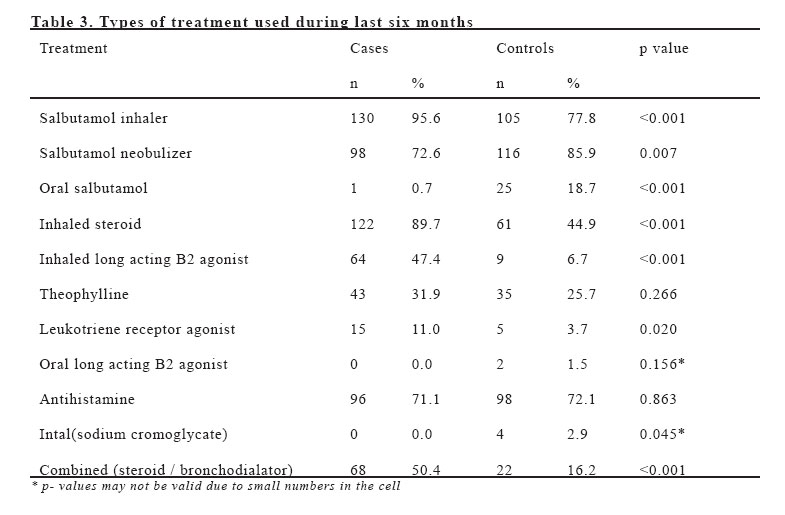
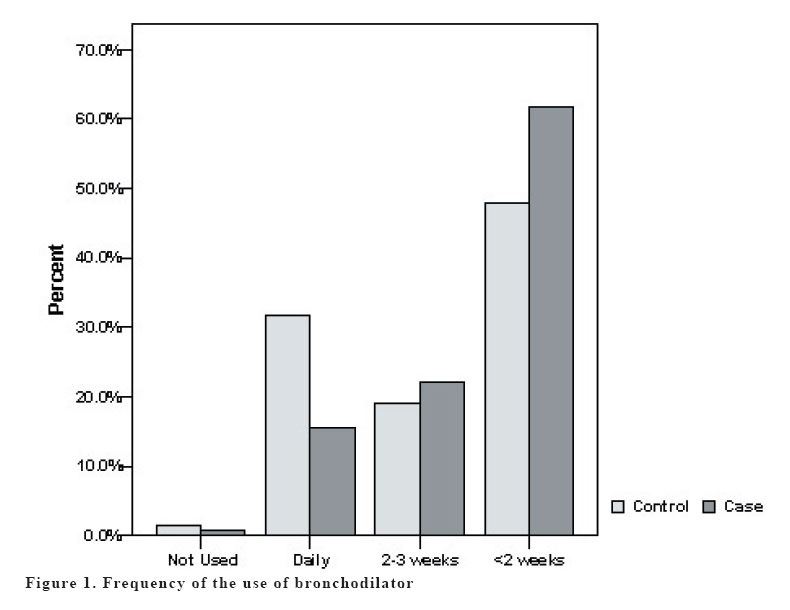
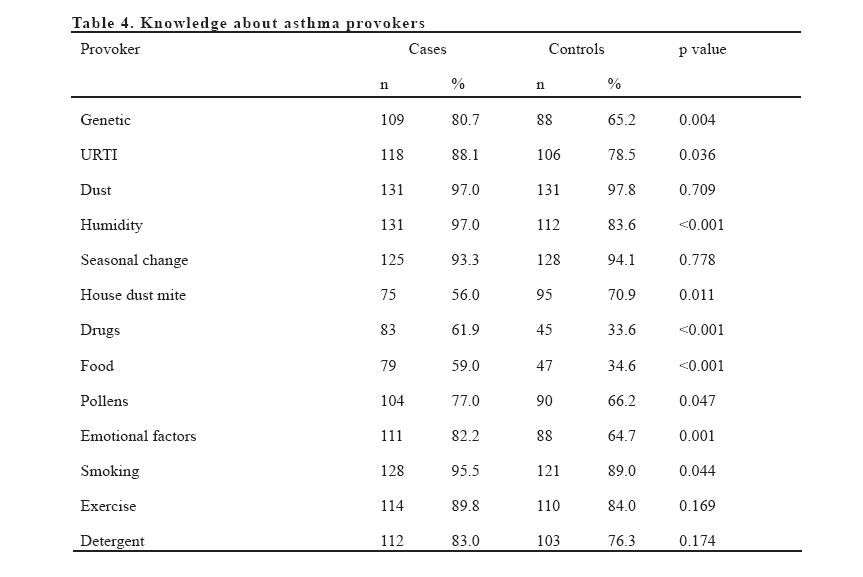
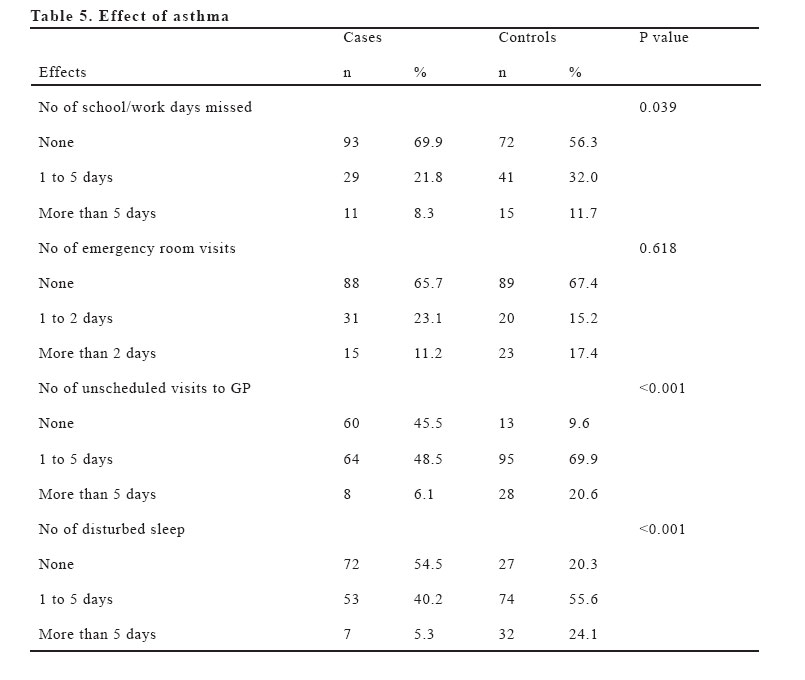
proper medication used and impact of asthma on life. Key words: Asthmatics, bronchodilator, neobulizer, primary care. INTRODUCTION Asthma is a major public health problem worldwide. It affects between 7 to 20 million people in the United States. Mortality and morbidity figures include approximately 5000 deaths and 100 million days of restricted activity annually. It is also responsible for more than 470,000 hospitalizations annually and an estimated 6 billion dollar in total medical cost (1). In Kuwait the annual cost of treating a case of moderate asthma is 562 US$. The lack of generic inhalers and inhaled steroids is the main reason for the high drug costs in Kuwait (2). Morbidity and mortality continue to increase despite the reversible nature of the disease and an expanding list of therapeutic agents. Asthma deaths can be traced to a number of factors including an underestimation of its severity, delays in starting treatment in acute exacerbations and unsatisfactory routine management. The international study of asthma and allergies in childhood (ISAAC) was set up to use standardized written and video questionnaires to study the prevalence of asthma, allergic rhinitis (AR) and eczema in different countries of the world. Kuwait ranked 13th among 56 countries in the prevalence of symptoms of asthma in children with a prevalence of current wheeze of 16% among Kuwaiti children[3]. The prevalence is higher than other countries in the Arab world where similar surveys were done namely Oman, Morocco and Lebanon. Studies have shown that many people with asthma remain sub-optimally treated when symptoms of asthma worsen. Many people admitted with acute asthma have had alarming symptoms for more than one week before admission (3). Asthmatics receive most of their treatment in general primary care clinics. Following the introduction of the government targets for health promotion and the chronic disease management plan, primary care clinics have been encouraged to set up clinics for the management of asthma (4). In Kuwait asthma clinics in general practice is limited and concentrated in few clinics where asthmatics are seen by a trained doctor, usually a family practitioner, once per week, e.g. 5 clinics in Hawalli health region and two in Capital health region. Protocols and clinical guidelines based on research evidence aim to standardize and improve processes and outcomes of care and stress on patient self management plan (1,5-10). Guidelines for treatment of asthma in general practice relate a series of step-ups in medication to indices of severity, eg. Peak flow recordings, symptoms such as wheeze and cough, night time waking, time off school or work or hospital admissions (4). Primary care studies show that guidelines are more acceptable and effective if they are developed locally by individuals who will be using them in conjunction with a practice-based education package. Several studies have examined the efficacy of a general practitioner and a nurse running asthma clinics. Clinics have a clear role in patient self-management education and clinic attendance reduces feelings of stigma and increases confidence in people with asthma. However, the type of intervention offered, who runs the clinic (general practitioner, nurse, or jointly run) and characteristics of clinic attenders, such as age and sex distribution, asthma severity and compliance with treatment, may influence clinic success in terms of improvement in asthma symptoms and reduced morbidity. Patient satisfaction is also an important outcome measure in health-care, predicting compliance and response to treatment (4,11). One study published in Kuwait 2002 showed that primary care centers in Kuwait lack essential medications for treating bronchial asthma. This undoubtedly affects the quality of care. In that study 33% of the centers surveyed had low dose and none high dose inhaled steroids. This makes the management of asthma very difficult for primary care physicians working in Kuwait (2). Asthma care in Kuwait is divided between the primary care centers, the regional general hospitals and a central specialized allergy centre (AL-Rashed Allergy Center) established in 1984, where patients from all over Kuwait with allergic diseases, including bronchial asthma, are referred for chronic management. As a result all the necessary medications are available in the allergy centre, while the general hospitals deal mainly with acute emergency department and in-hospital care. The policy of the Ministry Of Health is to confine relatively expensive medications to tertiary care centers such as the allergy centre and the general hospitals, which has created over-reliance of asthma patients on crisis management in the emergency departments. There is evidence that the rate of emergency department visits for asthma has been increasing in Kuwait (2). MATERIAL AND METHODS A survey study was conducted during the period of May 2005 to April 2006. The study focused upon the role of a structured programme of asthma care in general practice and the difference between asthmatic patients being followed in asthma clinic and asthmatic patients treated in ordinary general practice clinics. One hundred and thirty six cases were randomly selected from asthma clinics in Hawalli and Capital health areas according to the following criteria :-patients>12 years old, Kuwaitis, both sexes, and registered in asthma clinic and followed for at least 6 months. All cases were collected from Hawalli and Capital health regions since the other three health areas in Kuwait lack asthma clinics till April 2006. One hundred and thirty six controls were selected from general clinics in Hawalli, Capital and Ahmadi health areas. Any asthmatic being followed in a secondary or tertiary care unit for asthma was excluded from the control group. Also patients with chronic obstructive airway disease were excluded. Asthma was diagnosed based on recurrent attacks of cough and wheeze being relieved by bronchodilator. A questionnaire was designed based on the following broad sections: Socio-demographic characteristics which includes the patients age, sex, educational level, residence, weight, height, smoking status; and bronchial asthma history; asthma knowledge; effect of asthma on the patient; and patient satisfaction. The questionnaires collected were hand-checked for completeness before data entry and analyzed using appropriate statistical tests. The analysis was done on SPSS (Statistical Package for Social Sciences, version 13.0). The descriptive statistics, frequencies and percentages, are used to describe socio-demographic characteristics. Pearson Chi-square test of independence was used to test the association of qualitative variables viz. patient symptoms, types of treatment used, knowledge about asthma provokers and effect of asthma among cases and controls. A value of p<0.05 was considered to be significant. RESULTS Table 1 summarizes the baseline characteristics of the two groups. It is apparent that more than 70% of the patients among cases and controls were females (70.6% and 72.1%) respectively. The median age of the patients in the study group was 33 years ( 26.8) and the median age of the patients in the control group was 34 years (± 23.5). Educational status of the participants showed that the proportion of illiteracy was almost equal in both the groups. The patients of the control group were more educated (42.6% high school & 22.8% university and above) than in the case group. The highest percentage of cases was educated to elementary or intermediate level 43.3%. The percentage of smokers among cases was found to be 8.1% and among controls 11.8%. Table 2 compares the patient symptoms during the last 6 months namely persistent day cough, chest tightness, exercise intolerance, nocturnal symptoms, symptoms between the attacks and wheeze. All the previous symptoms were significantly less among cases compared to controls (p<0.001). Table 3 demonstrates the details of medications taken by the cases and controls during the last six months. Use of salbutamol inhaler, inhaled steroid, inhaled long acting B2 agonist, combination therapy and leukotriene receptor antagonist, were significantly more among cases (p<0.001, p<0.05). No significant difference was found between cases and controls in the use of theophylline, oral long acting B2 agonists and antihistamine. Use of oral and neobulized salbutamol were significantly reduced in cases compared to controls, (p<0.001) and none of them in the case group used sodium cromoglycate. The patients were asked about the number of hospital admissions they had in the past six months. Of the 136 cases, 129 patients (94.9%) reported that they had no admissions, 2.2% of them were admitted once and 2.9% of them were admitted more than once. Among controls 120 patients (88.2%) had no admissions in the past six months, 13 patients (9.7%) stated that they had been admitted once and the rest of them had two or more admissions. A statistically significant difference was also found between cases and controls in terms of systemic steroid used for the last six months, 28.9% of the cases used systemic steroid at least once compared to 16.4% of controls (p = 0.025). Using systemic steroids more than once, on the other hand, was more obvious in the control group (p < 0.05). Figure 1 shows the frequency of using bronchodilator between cases and controls which demonstrated that 31.6% of controls used bronchodilator daily compared to 15.4% of the cases. It showed also that most of the cases 61.8% had less than two attacks per week compared to 47.8% of controls. The availability of nebulizer, spacer and peak-flow meter (PFM) was tested. Only PFM was significantly available more in cases, 26.7% compared to controls, 3% (p<0.001) When testing both groups about their knowledge about asthma definition 27.9% of cases had the correct answer of (inflammation in addition to bronco-constriction, compared to 11% of the controls (p=0.002). Table 4 demonstrates the difference in terms of patient knowledge about asthma provokers. Cases were significantly more knowledgeable about some provokers namely, genetic, upper respiratory tract infections, humidity, drugs, foods and emotional factors (p<0.05). Other factors were not significantly different There was significant difference in terms of having leaflets about asthma, 83% of cases compared to 8.1% of controls (p=0.001). The presence of written management plan was also statistically significant 41.5% of cases compared to 5.9% of controls (p<0.0001). Among the different inhalers used metered dose inhaler (MDI), turbohaler and discus, the MDI was mostly used 69.9% controls and 39.3% cases. Using combined inhalers (two or more) was more obvious in cases than controls (p<0.001). When the technique of using inhaler was tested there was significant difference between cases and controls, 85.9% of the cases used their inhaler right compared to 42.5% of controls (p<0.001). About the use of (PFM), 88% of the control did not use it before while only 12.8% of cases did not have access to it. More than 75% of cases used it correctly compared to controls (6%), p<0.001. Although most cases and controls were satisfied about their symptoms control (54.1% and 61.8% respectively; 21.3% of controls were dissatisfied compared to only 5.9% of cases (p<0.001). Table 5 demonstrates the difference between cases and controls in terms of a number of school/work days lost, number of emergency room (ER) visits, number of unscheduled visits to the GP and the average number of disturbed sleep during last month. Among cases 30.1% of them missed school or work days, while 43.7% of controls missed these days p<0.05. Regarding ER visits 17.4% of controls visited ER more than two times during last 6 months, while 11.2% of cases visited ER more than two times during last six months. But that difference was not significant. Much less cases had unscheduled visits to GP during last six months when compared to controls,(45.5% & 9.6% respectively) p<0.001. Cases were more controlled than controls during night period and that difference was statistically significant p<0.001. DISCUSSION It appears that patients enrolled in Asthma clinic were superior significantly over asthmatic not in asthma clinics in most of the items tested, e.g. asthmatic in asthma clinic were more knowledgeable about the definition of asthma where inflammation plays an important role(12,13). This reflects their compliance on anti-inflammatory medication and hence more symptoms control. Knowledge was also obvious in identifying some of the provoker factors namely - genetic factors, upper respiratory tract infections (URTIs), pollens, smoking, humidity, drugs, foods and emotional factors. This reflects the importance of avoiding these factors as possible in order not to have new attack or to have milder ones. When tested for the medication used during the last six months, oral bronchodilator was significantly less in cases (p<0.001). This reflects that unnecessary medication is not used in asthma clinics and patients have less fear from the inhaled steroid. Inhaled steroids and inhaled long acting B2 agonists were used significantly by patients in asthma clinics than by controls. This reflects that clinicians in asthma clinics are aware of the stepping system for asthma management and indicates less fear from inhaled steroid. . This in terms reflect better control of asthma. It appears also that patients enrolled in asthma clinic were more proficient in using the inhaler (p<0.001). This reflects the knowledge of asthma clinic clinicians about the impact of faulty inhalation on the control of asthma, so more time is spent for teaching and rechecking during subsequent visits, this result is consistent with other studies (14). The measures of utilization of acute medical services e.g. ER and hospital admissions are more likely to reflect real improvements in asthma morbidity. Indeed, from a clinical perspective, the reduction in hospital admissions and emergency department visit is also likely to reflect a reduction in the risk of mortality as both are recognized risk factors for asthma mortality(9). In our study the difference between cases and controls in terms of using the acute medical services did not reach significance and this is in contrast with other studies (9,15,16). This might be attributed to the fact that the patients with acute attack usually go to the primary care clinic which is a walk-in clinic and now many clinics in Kuwait open for 24 hours. Another factor might be due to large number of patients in Kuwait have neobulizer at home so they manage themselves personally without requirement for ER. It was also found that some patients in asthma clinic had written self management plan which depends on their own stepping of medication depending on their symptoms and PFM readings. This reflects the patient awareness of their symptoms and their responsibility towards their disease and are less passive and dependable on their physicians. This of course decreases the frequency of acute attacks and their severity inconsistent with other studies (17). In conclusion, although the use of potent anti-inflammatory medications increases the cost of asthma medications at primary care level, it reduces the total health cost by reductions in other medical expenditure. So we recommend that stronger anti-inflammatory medication become available at primary care and to be guarded under rules to prevent the misuse of these medications. In addition, we recommend proper training of primary care physicians in long-term management of asthma patients. This will improve overall asthma care in Kuwait. The expanding of asthma clinics should be used as an opportunity to improve asthma care at primary care level. ACKNOWLEDGMENT We would like to thank Dr.Naser Behbehani, Consultant Respiratory physician in Kuwait Chest Hospital, for his support and for providing us with related articles. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06034t2.jpg] [gm06034t3.jpg] [gm06034t5.jpg] [gm06034t1.jpg] [gm06034f1.jpg] [gm06034t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}