 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
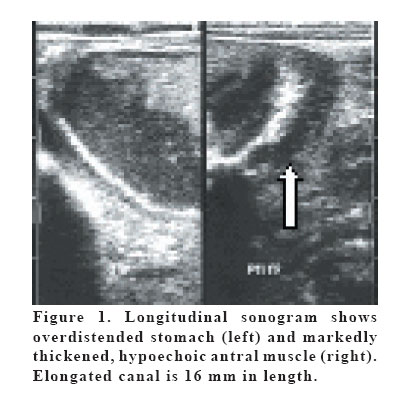
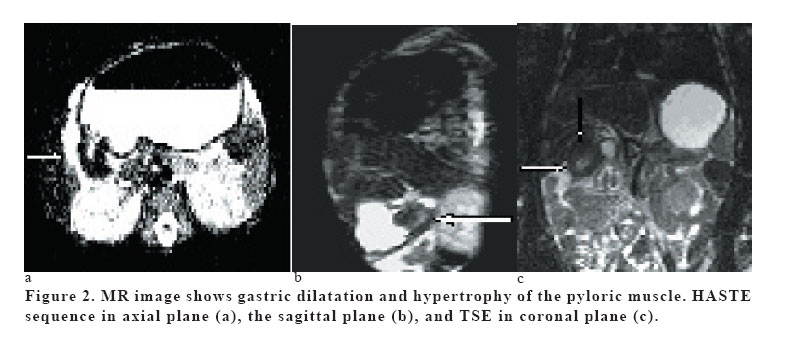
European Journal of General Medicine, Vol. 3, No. 4, 2006, pp. 186-189 HYPERTROPHIC PYLORIC STENOSIS MR FINDINGS Halil Arslan1, Ali Bay2 , Osman Temizöz1 ,Ömer Etlik1, Burhan Köseoğlu3, Erol Kisli4 Yuzuncu Yil University Faculty of Medicine, Department of Radiology1 , Pediatry2 and Pediatric Surgery3 and General Surgery4 Van, Turkey Code Number: gm06040 Infantile hypertrophic pyloric stenosis (IHPS) is a condition affecting young infants, in which the antropyloric portion of the stomach becomes abnormally thickened and manifests as obstruction to gastric emptying. The clinical diagnosis hinges on palpation of the thickened pylorus, or 'olive.' Abdominal palpation is accurate but not always successful, in such cases, radiologic examinations including US or MRI can be performed. US is the first choice of imaging modality. Unfortunately, in case of difficulty by the sonographic diagnosis of IHPS such as overlying bowel gas, MRI could be useful for the diagnosis. Key words: Infantile hypertrophic pyloric stenosis, MRI INTRODUCTION Infantile hypertrophic pyloric stenosis (IHPS) is a condition affecting young infants, in which the antropyloric portion of the stomach becomes abnormally thickened and manifests as obstruction to gastric emptying. The clinical diagnosis hinges on palpation of the thickened pylorus, or 'olive.' Abdominal palpation is accurate but not always successful, depending on factors such as the experience of the examiner, the presence of gastric distention, and a calm infant. In patients in whom clinical examination is unsuccessful, modern imaging techniques are highly accurate in facilitating the diagnosis. The radiologist, therefore, plays a key role in the initial care of these infants and the appropriate surgical referral. Fluoroscopy, gray scale ultrasonography (US) and Doppler US could be used in the diagnosis of IHPS. There are a lot of studies in the literature performed with these modalities (1-5). The purpose of this study is to show and describe (magnetic resonance imaging) MRI findings in IHPS. CASE A 4-month-old male infant, complaining of projectile vomiting applied to pediatrics clinic. There was no significant finding in the physical examination and the patient was referred to radiology department for the suspicion of upper gastrointestinal abnormality such as pyloric stenosis. The patient was examined with US, performed with a standard fashion in the longitudinal and transverse planes with a linear and convex transducer operating at a 3-8 MHz frequency (Siemens Sonoline Adara, Germany). The US examination could be performed with difficulty due to overlying bowel gas. Despite obscuring bowel gas, we could assess the pyloric canal with different positioning of the probe. The thickness of the pyloric muscle and the length of the pylorus were measured. Muscle thickness was measured on both longitudinal and transverse sections of the pylorus. The muscle thickness was 4.5 mm and the length of the hypertrophied canal was 16 mm, which was typically described as 'elongation' of the pyloric canal termed the string or double-track sign. The stomach was overdistended (Figure 1). There were no other findings in US examination. After the US examination the patient was moved to MR room and MR examination was performed in order to get more diagnostic findings for IHPS (Magnetom Symphony, Siemens, Germany). After the sleeping, the MR images were obtained in the axial, sagittal or coronal plane. We evaluated the patient with T2-weighted half-Fourier single-shot turbo spin-echo (HASTE) sequence, true fast imaging in the steady-state procession (true-FISP) sequence and fast spin-echo (FSE) T2-weighted sequence followed by the acquisition of 'spoiled' 2D gradient echo T1-weighted sequence (FLASH, fast low-angle shot). All images showed distended gastric lumen and hypertrophic pyloric muscle with isointensity compared to muscle tissue. HASTE images were better than other sequences showing the abnormal pyloric muscle as a low signal intensity (Figure 2).The length and thickness of the hypertrophic pyloric muscle in MR examination was similar with US examination. Therefore, MR imaging confirmed sonographic data. Then the patient was operated using the hypogastric approach. The diagnosis was confirmed with surgically and pathologically and the patient was discharged from the hospital without any complication. DISCUSSION The diagnosis of IHPS is initially suggested by the typical clinical presentation. Palpation of the hard muscle mass, or olive, is diagnostic but is often challenging and time consuming. In cases in which physical examination are unsuccessful, other methods must be used to establish the diagnosis. Several techniques involving insertion of a nasogastric tube and endoscopy have been proposed over the years (1-7). However, the invasiveness of these procedures does not seem to justify their use when other diagnostic methods are available. There was no significant finding in clinical examination and we did not prefer to evaluate with these kind of invasive techniques. Typically, infants with IHPS are clinically normal at birth; during the first few weeks of postnatal life, they develop nonbilious forceful vomiting described as 'projectile.' Non-bilious emesis is the most important symptom which is intermittent or after each feeding. Gastric outlet obstruction leads to emaciation and, if left untreated, may result in death. IHPS affect 0.5 to 3.0 per 1000 live births. The etiology is unclear, but family history, sex distribution and environmental factors seem important and might indicate a genetic role. The male-to-female ratio is approximately 4:1 with reported ratios ranging from 2.5:1 to 5.5:1 (1-3). Over the subsequent 4 decades, upper gastrointestinal barium examination became widely used in cases in which palpation of the olive was unsuccessful at clinical examination. The barium examination provides indirect information regarding the status of the antropyloric canal based on the morphology of the canal lumen as outlined by contrast material. The examination may be time consuming, particularly in infants with high-grade obstruction, because it necessitates awaiting the passage of contrast material through the obstructed canal. Fluoroscopy time and, therefore, radiation exposure may be prolonged. On the other hand, failure of relaxation of the antropyloric canal, also known as pylorospasm, may be difficult to differentiate from IHPS (8). Until wide use of ultrasound in diagnostic procedures took its part, the only relevant procedures to diagnose IHPS were clinical examination and X-ray of gastroduodenal tract. In 1977, Teele and Smith published a report on five cases in which a correct diagnosis was rendered after using articulated-arm B-mode sonography; this initiated a proliferation of articles on the sonographic diagnosis of IHPS (9). Sonographic examination demonstrates the thickened prepyloric antrum bridging the duodenal bulb and distended stomach. In infants with IHPS, the stomach is distended to a variable degree. Three main ultrasonographic parameters can be used: pyloric muscle thickness, pyloric diameter, and pyloric length. It was reported that a length of the pyloric canal 20±6 mm, a diameter 13.6±2.5 mm, and a muscle thickness 4.1±1 mm are diagnostics for hypertrophic pyloric stenosis (1,4,10,11). In our case, the stomach was overdistended and pyloric muscle thickness and length were 4.5 mm and 16 mm respectively. Doppler US also can be used in diagnosis of IHPS showing passage of liquid through the narrowed pyloric canal and increased blood flow to the antropyloric canal (5,6). We did not performe the Doppler US in diagnostic procedure. There is only one MRI study in the literature performed in IHPS (12). It may not be necessary to evaluate IHPS with MRI. It is expensive and evaluation of the gastrointestinal tract especially in infants is not so easy with MRI because of the known reasons. But, in spite of the reliability of the procedure is very high, there are some limitations in US. It is operator dependent, and the learning curve is step. Overlying bowel gas by the transverse colon or gastric distension may occasionally obscure the gastric antrum and hinder the sonographic diagnosis of hypertrophic pyloric stenosis (13). In our study, bowel gas obscured the pylorus and the diagnosis was difficult. For all these reasons, other modalities without containing X-ray such as MRI might be necessary in the evaluation of IHPS. As a result, in experienced hands, sonography should be used as primary imaging modality in diagnosis of IHPS. In case of difficulty by the sonographic diagnosis of IHPS such as overlying bowel gas by the transverse colon or gastric distension obscuring the gastric antrum, MRI could be useful for the diagnosis. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06040f1.jpg] [gm06040f2.jpg] |
| |||||||||

{kind=link}
{kind=link}