 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 3, No. 4, 2006, pp. 193-196 SPINAL ENTEROGENOUS CYSTS IN INFANTS Nurullah Yüceer¹, Erdener Ozer2, Meral Koyuncuoglu2 Dokuz Eylul University Faculty of Medicine, Departments of Neurosurgery1 and
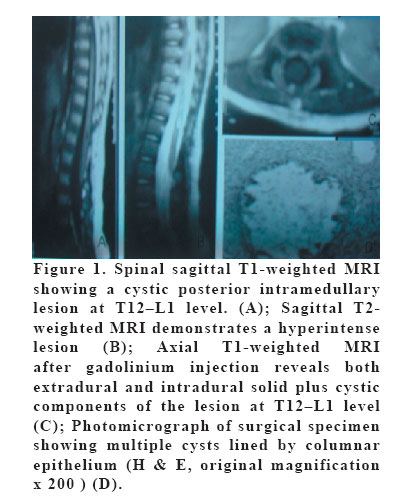
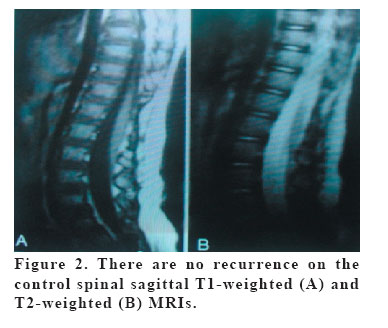
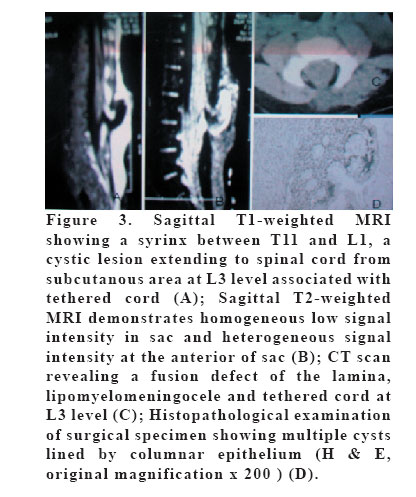
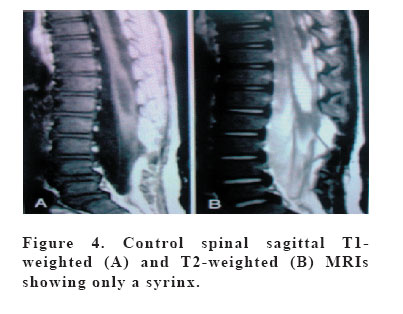
Pathology2, İzmir, Turkey Code Number: gm06042 Intraspinal enterogenous cysts are very rare congenital cysts of endodermal origin, and tend to occur in anterior spinal intradural space. The diagnosis is usually established during the first or second decade of life. Those cysts are frequently associated with vertebral or spinal cord anomalies and dual malformation with mediastinal or abdominal cysts. We report two infants of posterior spinal enterogenous cyst in this study, one thoracolumbar (T12-L1) and one lumbar (L2-L4) presenting with features of subcutaneous lesion of posterior spinal. In one magnetic resonance imaging (MRI) showed a cystic mass extending to posterior intramedullary from subcutaneous localization at T12-L1, and in the other MRI demonstrated a syrinx extending from T11 to L1, tethered cord syndrome associated with a meningocele sac between L2 and L4. The cystic lesions in the patients were removed. The postoperative courses were uneventful. The patients appeared well after six years and four years of follow-up, respectively. Successful treatment requires early recognition of those cysts and their associated abnormalities. Key words: Enterogenous cyst, Infant, Magnetic resonance imaging, Spinal cord INTRODUCTION Spinal enterogenous cysts (EC) are rare congenital lesions deriving from endodermal inclusions and that tend to occur in anterior spinal intradural space. ECs are central nervous system (CNS) cyst lined by endothelium primarily resembling that of the gastrointestinal (GI) tract, or less often, the respiratory tract. Spinal ECs may have a fistulous or fibrous connection to the GI tract and some call these as endodermal sinus cysts. These are thought to occur as a result of incomplete developmental separation of the notochord from the primitive gut (1,2,3). ECs are more commonly found in the lower cervical or thoracic intradural extramedullary (1,3), and in the ventral area of the spinal cord (1,3,4,5,6). This report describes two infants with intramedullary placed EC extending to dorsal intradural area from subcutaneous area at T12 –L1 level and at L2–L4 level, respectively. CASE 1 An 6-month-old girl infant was admitted to our clinic due to lower thoracic subcutaneous lesion. Her physical examination showed a soft mass of the subcutaneous area at the lower thoracic level. Neurological examination was normal. Cranial computerized tomography (CT) scan was normal. Spinal CT scan showed a fusion defect of lamina and dorsal intramedullary hypodense lesion at T12-L1 level. Magnetic resonance imaging (MRI) revealed a lesion hypointense on T1-weighted images and hyperintense on T2-weighted images at posterior intramedullary localization. The lesion included both cystic and noduler components. In addition, it is extending intramedullary from subcutaneous area at T12–L1 level (Figure 1A,1B and 1C). Preoperative somatosensorial evoked potential (SEP) examination could not be performed. Urodynamic studies were normal. CT and MRI studies were followed by microsurgical removal of the lesion. T12-L1 level was explored. Firstly, both subcutaneous and epidural lipoma were excised. Epidural lipoma was extending to intradural area at EC localization. Then, both intradural lipoma and intramedullary cystic lesion were completely excised. Postoperative course was uneventful. Neurological examination was normal. Pathological examination confirmed an EC (Figure 1D). Six years later, patient’s neurological examination was normal. Urinary incontinence or encopresis were absent. Somatosensorial evoked potential examination was normal at the postoperative follow-up. There was no recurrence on control MRI (Figure 2). CASE 2 This 2-month-old girl infant suffered a lomber subcutaneous mass in 4x4 cm size. She had a meningocele mass without any cerebro-spinal fluid (CSF) leak at the lomber level and a dermal sinus tract at the sacral level. Neurological examination was normal. Spinal CT scanning revealed a fusion defect of lamina and a meningocele sac at the L3 level (Figure 2A). MRI studies demonstrated a syrinx extending from T11 to L1, tethered cord syndrome associated with a meningocele sac between L2 and L4 (Figure 3A,B). Spinal CT scanning revealed a fusion defect of lamina and a meningocele sac at the L3 level (Figure 3C). Cranial MRI was normal. Preoperative somatosensorial evoked potential examination could be no performed. Urodynamic studies were normal. At operation lomber meningocele sac was explored and an intradural component of both CSF and lipoma were observed. There were extending to dorsal of spinal cord both intradural lipoma and cystic lesion. Both lipoma and cystic component were totally excised and untethering was succeed. In addition, filum was sectioned and sacral dermal sinus tract was excised. Postoperative course was uneventful. Neurological examination was normal. Histopathological examination showed an EC associated with lipomyelomeningocele (Figure 3D). Four years after the operation, her neurological examination was normal. SEP examination was normal at the postoperative follow-up. The patient had no urinary incontinence or encopresis. There was no recurrence on control MRI (Figure 4). DISCUSSION ECs are usually simple cysts lined by cuboidal columnar epithelium and mucin secreting goblet cells. Less common types of epithelium described include: stratified squamous and pseudostratified columnar, and ciliated epithelial cells. Mesodermal components may be present, including smooth muscle and adipose tissue, and some have called these teratomatous cysts which is not to be confused with teratomas which are true germinal cell neoplasm (1,3,4). Spinal ECs have been classified topographically into two types: anterior-lying lesions without vertebral anomaly usually occurring in the cervical region, and lesions posterior to the cord often associated with spinal defects. Spinal ECs usually locate ventral intradural extramedullary (1,3,4,7,8). Intramedullary EC is reported rarely in the literature (1,2,9,10,11,12,13,14,15). Dorsally placed spinal EC is very rare (16), as in our cases. Our cases presented dorsally placed intramedullary ECs of the lower thoracic and lomber spine. Spinal ECs may occur either alone or in the context of a complex malformative disorder including typical vertebral and cutaneous abnormalities such as diastematomyelia, dorsal fistula, lipoma and syringomyelia. (1,4,17). Our one case had only spina bifida associated with the EC. However, the other case had spina bifida, syrinx, intradural lipoma, meningocele, dermal sinus tract and tethered cord syndrome associated with the EC. Clinical symptoms and signs most commonly present during the first decade of life. Pain or myelopathy are the most common presentations in older children and adults. Neonates and young children may present with cardiorespiratory compromise from an intrathoracic mass or cervical spinal cord compression (3,6,8,18,19). ten Donkelaar and et al (8) reported an infant with spinal intradural enterogenous cyst who led to the death due to progressive respiratory failure. Meningitis may occur from the fistulous tract, especially in new-borns and infants. Our cases admitted to our clinic due to a lower thoracic subcutaneous lesion, and a lomber subcutaneous mass, and neurological examinations were normal. The rarity of these lesions makes preoperative diagnosis difficult. CT and especially MRI may help in diagnosis of the spinal ECs (3,16). MRI studies show an appearance of hyperintense to cerebrospinal fluid on T1-weighted sequences and an appearance of isointense on T2-weighted sequences (20). MRIs of our cases demonstrated a mainly hypointense lesion on T1-weighted images, and hyperintense on T2-weighted images. Microsurgical complete removal of spinal EC usually reverses the clinical symptoms and signs (4,16). An adherent capsule may prevent complete resection of ECs, which predisposes to delayed recurrence and mandates long-term follow-up. The presented infants were neurologically normal six years and four years after the operation, respectively. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06042f3.jpg] [gm06042f2.jpg] [gm06042f4.jpg] [gm06042f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}