 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
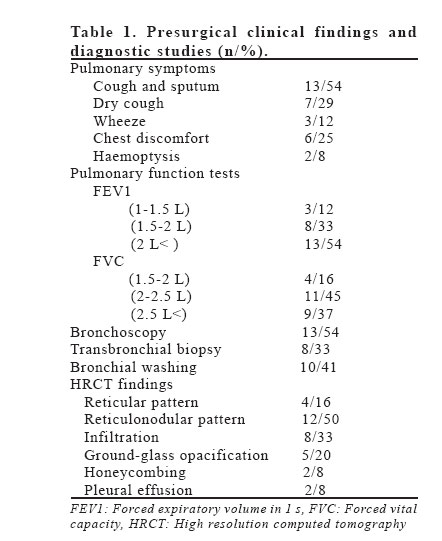
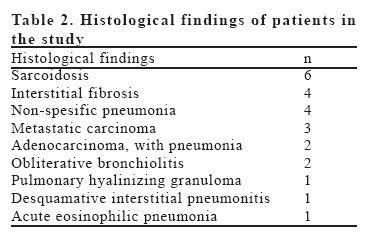
European Journal of General Medicine, Vol. 4, No. 1, 2007, pp. 16-18 IMPORTANCE OF OPEN LUNG BIOPSY IN PATIENTS SUSPECTED INTERSTITIAL LUNG DISEASE Hıdır Esme1, Murat Sezer2, Okan Solak1, Önder Şahin3 Afyon Kocatepe University, Faculty of Medicine, Departments of Thoracic Surgery1, Pulmonary Medicine2 and Pathology3, Afyon, Turkey Code Number: gm07004 Aim: The purpose of this study was to review the role of surgical lung biopsy techniques in patients with suspected interstitial lung disease to determine the outcomes in terms of diagnosis and management. Key words: Open lung biopsy, interstitial lung disease, morbidity INTRODUCTION Interstitial lung disease (ILD) is a generic term representing a heterogeneous group of lung diseases classified together because of several common features (1). Although high resolution computed tomographic (HRCT) scan of the chest may reduce the proportion of patients undergoing surgical lung biopsy, surgery may still be needed to establish an accurate diagnosis, to identify potential treatable causes and to rule out other processes (i.e. infection and malignancy) (2). The decision to perform lung biopsy in patients with ILD is based on the likelihood that pathological examination of the tissue obtained will yield specific information about the cause of the disease process and whether this information can be used to alter the treatment being received by the patient (3). Surgical lung biopsy includes open and video-assisted thoracic surgery (VATS) procedures. In this study, we reviewed the role of surgical lung biopsy techniques in patients with suspected ILD to determine the outcomes in terms of diagnosis and management. MATERIALS AND METHODS Twenty-four patients with suspected diagnosis of ILD on clinical and radiological grounds who had been referred to our department between July 2003 and April 2006 were included in this study. Patients with a solitary nodule or other focal pulmonary processes were excluded. Twenty open lung biopsies had been performed under general anesthesia. Limited anterior thoracotomy, usually through the fifth intercostal space, had been used. Four patients had undergone VATS. Tissue samples had been obtained from the mostly involved lung area, normal appearing areas, and transitional areas, based on the appearance on HRCT scan. Frozen section examination was performed when a tumor lesion was suspected during the operation. Most patients had previously been investigated with chest X-ray, HRCT or CT scan, spirometry, bronchoscopy, transbronchial biopsy, bronchial washings, sputum specimen for culture and cytological examinations prior to surgery. Data were collected from patients’ medical records: age, sex, previous diagnostic studies, biopsy type, site, and number, histopathology, diagnostic yield, change of therapy, the post-operative length of hospital stay, mean chest tube drainage duration, and post-operative morbidity and mortality were noted. RESULTS During the 3-year period, 24 patients had been referred to our department for surgical lung biopsy. Of these 24 patients, 17 were men and 7 were women, with a median age of 51.5 years. Table 1 lists presurgical clinical findings and diagnostic studies. Open lung biopsy had been performed in 20 (83.4%) and VATS had been performed in 4 (16.6%) patients. In 2 patients surgical procedure had changed from VATS to open surgery because of pleural adhesions. Samples had been obtained from lower lobe in 20, upper lobe in 8 and middle lobe in 2 patients. One to three samples from each patient, with a total of 42, had been obtained. All the lung samples were adequate in amount and quality for histopathological examination. Nine patients (37.5%) had received a histological diagnosis not consistent with ILD. In these nine patients (Non-spesific pneumonia in four patients, metastatic carcinoma in three, and adenocarcinoma with pneumonia in two), subsequent management had altered. The list of all histopathological findings is shown on Table 2. Mean post-operative length of hospital stay was 3.6 days (2-15 days). Mean chest tube drainage duration was 2.1 days. There was no in-hospital mortality in this series of patients. Post-operative complications had been observed in 2 patients who had received VATS procedure. Two patients had had pneumothorax with persistent air leakage for more than one week, which later had resolved with conservative treatment. Post-operative hemorrhage had occurred in one patient who had undergone open lung surgery. This patient had received blood transfusion but re-thoracotomy had not been required. DISCUSSION Patients with ILD are challenging to treat. Many patients have inadequate information about the disease process; an imprecise diagnosis, unsatisfactory treatment, or unacceptable side effects associated with therapy, and poorly controlled symptoms of progressive illness. Establishing an accurate diagnosis is essential so that the patient and his/her family can be provided with reasonable expectations about the prognosis and effects of therapy (3). Open lung biopsy provides sufficient material for histopathological diagnosis in most of cases (2). Our results also demonstrated efficacy of open lung biopsy in the diagnosis of ILD. Most physicians prefer a trial of steroid therapy instead of diagnostic interventions for these patients. Possible reasons for this preference include advanced age and poor performance status of the patient, invasiveness of surgical biopsy for both the physician and the patient, distrust to pathological diagnosis and the thought that the pathological finding would not change the treatment (4). In fact all the current treatments have severe potential adverse effects. It seems not wise to expose an undiagnosed patient to such a risk. Various reported series show a change in management based on biopsy results in 27–73% of patients undergoing this procedure for ILD (3,5,6). As a result of histopathological examination the initial clinico-radiological diagnosis and subsequent diagnosis had changed in 9 (37.5%) patients in our study. Controversy exists regarding the methods and indications for lung biopsy. The sample size and the number of sites that undergo a biopsy vary considerably. Some surgeons prefer to biopsy a single site, whereas others sample several different areas; the latter approach is strongly recommended (7). In our study group, the preoperative HRCT scans had been reviewed and biopsy samples had been obtained from multiple separate areas, including areas of affected lung with active disease, normal appearing areas, and, most importantly, the transitional areas whose gross appearance is between the other sites. Several studies in the literature have shown that multiple biopsy specimens obtained from different areas of lung are clearly superior to a single biopsy specimen (8-11). In conclusion, open lung biopsy can safely be performed in patients with suspected ILD. The morbidity and mortality are low, length of hospital stay and chest tube drainage duration are relatively short. It alters the diagnosis and management in a significant number of patients. Although surgical lung biopsies remain the most sensitive and specific test available for many patients with ILD, they should be used when a definitive diagnosis cannot be established with available clinical and radiographic data and less invasive diagnostic procedures. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07004t2.jpg] [gm07004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}