 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
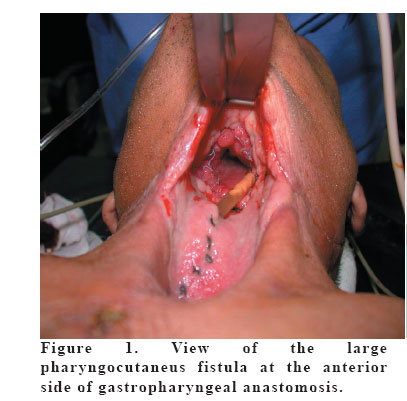
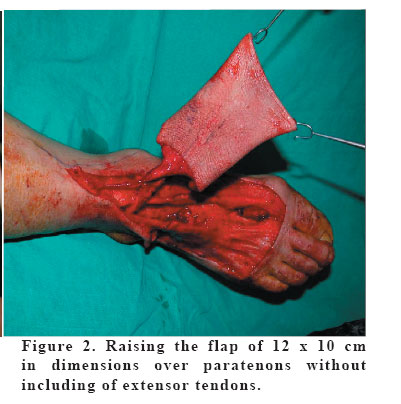
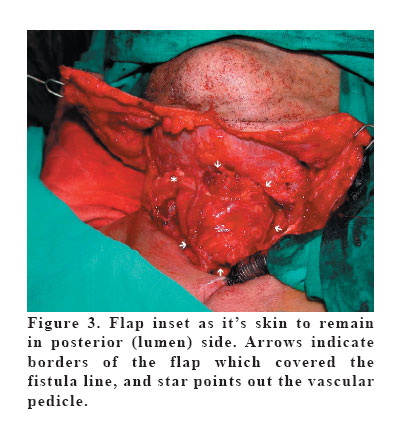
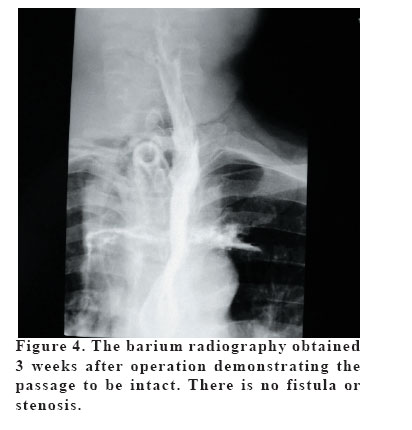
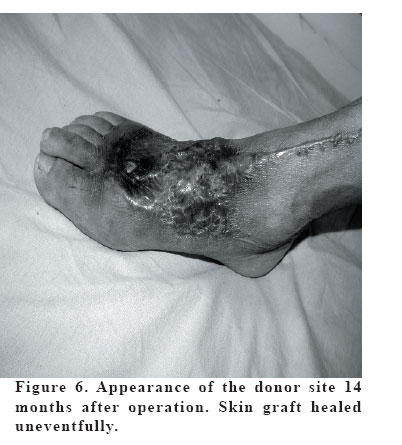
European Journal of General Medicine, Vol. 4, No. 1, 2007, pp. 39-43 REPAIR OF A LARGE PHARYNGOCUTANEOUS FISTULA WITH THE FREE DORSALIS PEDIS FLAP Önder Tan1,Bekir Atik2 , Duygu Ergen1 Ataturk University Medical Faculty, Department of Plastic and Reconstructive Surgery¹, Erzurum, Yuzuncu Yil University Faculty of Medicine, Plastic and Reconstructive Surgery2 Van, Turkey Code Number: gm07009 Postoperative pharyngocutaneous fistulas are the relatively frequent complications of total laryngo-oesophagectomy. Despite various treatment strategies have been mentioned in the literature, ideal method for closure of the large pharyngocutaneous fistulas is still controversial. In this report we have succesfully closed a large pharyngocutaneous fistula with free dorsalis pedis flap after ablation of oesophageal cancer. Key words: Dorsalis pedis, flap, pharyngocutaneous fistula INTRODUCTION Repair of a pharyngocutaneous fistula after cancer resection is a challenge, particularly if the fistula is large and involves half or more of the circumference of the pharyngo-oesophagus. Such a large fistula usually results either from wound breakdown after total laryngectomy or necrosis of the transferred tissue that was used for reconstruction of the pharyngo-oesophageal defect (1). Althought the clinical presentation varies, they are frequently life-threatening. Despite various treatment strategies including local, regional or distant flaps have been mentioned in the literature, ideal method for closure of the large pharyngocutaneous fistulas is still controversial and there is no agreement among the surgeons. The microvascular free flaps such as the radial forearm flap, island trapezius flap, free jejunal interposition and gastric pull-up transfer have been the transplants predominantly used for reconstruction of the hypopharynx and cervical esophagus defects (2). Free flaps are the established and reliable methods in surgical armamentarium. We have succesfully closed a large pharyngocutaneous fistula with the free dorsalis pedis flap after ablation of oesophageal cancer. CASE A 56-year-old man presented with dysphagia and odynophagia of 2 months. The disphonia had been also added for a last week. He was a smoker for 30 years. On physical examination jugular and submandibular lymphadenopathies were palpated. The computed tomography of the thorax and larynx revealed the tumoral mass in the upper third of the esophagus. The histopathological diagnosis was establish as the squamous cell carcinoma with punch biopsy under esophagoscopy. The patient underwent total laryngo-oesophagectomy, gastric pull-up procedure, bilaterally Type IIII modified radical neck dissection and total tyroidectomy. However, a pharyngocutaneus fistula was developed at the anterior side of gastropharyngeal anastomosis 20 days after operation (Figure 1). We decided to repair the fistula with a bilateral platysma muscle flaps. Although the complete repair was achieved, dehiscense occured again in fifth day postoperatively. Then, the free dorsalis pedis flap was planned. Under general anesthesia operation area and right foot as the donor region were prepared. A flap of 12 x 10 cm in dimensions was planned and suitable drawing was made. The right facial artery and it’ s concomitant vein at the recipient side were determined and prepared. By starting the dissection from distal to proximal under pneumonotic tournique, the flap was raised over paratenons without extensor tendons (Figure 2). The first dorsal metatarsal artery as a terminal branch of the dorsalis pedis artery was found, tied and included into the flap between the heads of first and second metatarses. At the proximal side the dorsalis pedis artery, it’s two concomitant veins and saphen vein were dissected 15 cm proximally and included in the flap. After checking the perfusion of the flap, all the vessels were clamped and the flap was divided. While a team repaired the donor region by split-thickness skin graft, another team performed microvascular anastomosis at the recipient site. The dorsalis pedis artery and big one of the concomitant veins were end-to-end anastomosed to the facial artery and vein. It was observed that the flap was perfused well and bleeding from other veins was confirmed. Flap was inset as it’s skin to remain in posterior (lumen) side and sutured with 4/0 polyglycolic acid watertightly through the fistula line (Figure 3). The skin flaps of the neck were then sutured to each others over the dorsalis pedis flap. Any peroperative complication was not encountered. In barium radiography obtained three weeks after operation, the passage was uneventful and there was no fistula or stenosis (Figure 4). The nasogastric feeding tube was then removed and a clear diet was given orally (Figure 5). Soft and normal diet were started to give 6 and 10 weeks in postoperative period, respectively. Skin graft at the donor site healed uneventfully and the patient began to walk 15 days after operation. In follow-up of 14 months no complication was seen (Figure 6). DISCUSSION Postoperative pharyngocutaneous fistula is a relatively frequent complication of total laryngo-oesophagectomy that prolongs the hospitalizasyon of 2 to 3 weeks to many weeks or even months (3). Small or medium sized fistulas, especially in nonirradiated patients, usually close spontaneously with conservative therapy. When fistulas fail to close with conservative methods, debridment and flap closure are indicated. Surgical treatment has not yet been standardized and, at present , there is no consensus on an ideal flap preference for repairing complex lesions. Direct closure is often not possible for larger wounds, especially in radiation fields (4). Local procedures such as rhomboid flaps, rotation and transposition flaps, and lateral cervical flaps have been used (5). However, because of the random pattern vascular supply of these flaps, the failure rate has remained high and the risk of tissue necrosis after neck dissection and heavy radiation discourages their use (6). The Bakamjian flap, elevated from the deltopectoral region based on an axial vascularization coming from cutaneous branches of the intercostal arteries, has long been the flap of choice for closure of large pharyngocutaneous fistulas. However, it usually requires two reconstructive procedures and leaves major aesthetic sequelae (4). Sternocleidomastoid muscle flaps have been used for closure of nonmalignant fistulas (6). The pectoralis major flap can be used with or without a skin island. However, it is very bulky and is generally indicated in the cases of large substance loss in the pharyngolaryngeal area (4). Janssen and Thimsen suggested the use of a full-thickness flap involving the middle third of the lower lip based on the submental artery for full-thickness closure of cervical esophagocutaneous fistulas (6). However, the important drawback to this procedure is the aesthetic change in the central third of the lower lip. Fabrizio et al reported the use of the fasciocutaneous island flap pedicled on the superficial temporalis artery for the reconstruction of a pharyngocutaneous fistula in a patient. They used a skin graft for donor-site closure (7). The donor site morbidity was the most noticeable disadvantage of this flap. Other described techniques include the use of free flaps. Free intestinal flaps provide the ability to close larger fistulas in a one-stage operation (8). These flaps are particularly appropriate for circumferential reconstructions. However, these procedures can be quite extensive and necessitate to open the abdomen. The free radial forearm flap is a suitable alternative for reconstruction of the pharyngocutaneous fistulas (9). This flap, which is especially considered for non-circumferential (onlay) defects, has some advantages consisted of versatile use, a constant and safe pedicle, the thinnest and most pliable texture among all the flaps. However, it may leave a troublesome scar in donor site (10). Another major problem with this technique is that it sacrifices a major artery, radial artery, to the hand, when especially needed to a long vascular pedicle. Although problems following division of the radial artery are rare, some cases have been reported (11). In the present case, to avoid a conspicuous scar in forearm and not to sacrifice one of the major arteries of the hand, we preferred the analogous flap in lower extremity to radial forearm flap: the dorsalis pedis flap. The dorsalis pedis flap was initially described by McCraw and Furlow (12) in 1975 as a local transposition flap. Applications as a free flap were described by Ohmori and Harii (13) in 1976. Since then, it has been used to reconstruct defects in the head and neck, upper and lower extremity. However, to the best our knowledges, there is no specific report regarding the use of free dorsalis pedis flap for pharyngocutaneous fistulas in the literature. Several features of the dorsalis pedis flap, including its’ thinness, reliable vascularity, long vascular pedicle, and potential for inclusion of vascularized tendons have made it an attractive option for free-tissue transfer. However, donor-site complications such as healing slowly (14), prone to late breakdown and noticeable scar have consistently been reported (15). The frequent occurrence of donor-site problems has diminished popularity of this flap. We encountered no donor site complication and skin graft healed uneventfully in our case. In our opinion, the free radial forearm and dorsalis pedis flaps are the most suitable choices in the management of large pharyngocutaneous fistulas. Because the transferred tissue in this area is preferred to be adequately pliable and thin which affects the aesthetic and functional outcomes. On the other hand, we think that the free dorsalis pedis flap leaves relatively less conspicuous scar on the foot which may better accepted by the patients because of its’ less noticeable location, when compared with free radial forearm flap. In conclusion we propose the free dorsalis pedis flap as a good choice for large pharyngocutaneous fistulas because of its’ pliable and thin texture with less conspicuous scar in donor site. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07009f6.jpg] [gm07009f1.jpg] [gm07009f5.jpg] [gm07009f4.jpg] [gm07009f2.jpg] [gm07009f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}