 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
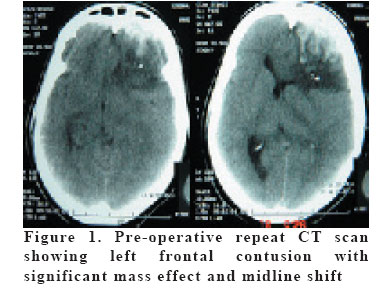
European Journal of General Medicine, Vol. 4, No. 1, 2007, pp. 44-46 PRE-CHIASMATIC NERVE INJURY FOLLOWING FRONTAL CONTUSION Amit Agrawal1, Lekha Pandit2, Vittal Nayak3, Srikrishna U4, Bobby Varkey4 K.S.Hegde Medical Academy, Departments of Neurosurgery¹, Neurology2, Ophthalmology3 and Radiology4 Mangalore, India Code Number: gm07010 A 41 year old female following decompression of post-traumatic frontal contusion was complaining of visual loss in ipsilateral eye. Clinical and imaging features were suggestive of compression injury to intracranial part of left optic nerve. We discuss and correlate clinical and imaging findings in this case of pre-chiasmatic nerve injury. Key words: Foster-Kennedy syndrome, optic nerve, frontal contusion, vision loss INTRODUCTION Head injury is a leading cause of visual impairment. Visual impairment may be due to the direct trauma to the eye or trauma can damage the intracranial optic pathways. However optic chiasm and the posterior segment of the optic nerve are the least affected parts (1). Prechiasmal vision loss due to intracranial optic nerve infarction has been reported in the setting of subdural haematoma and a rare entity (2). We discuss the clinical and radiological findings in a case of frontal contusion with pre-chiasmatic optic nerve injury who also had features of Foster-Kennedy syndrome. CASE A 41 year old female from rural south India presented 6 hours after fall from motorcycle with the history of loss of consciousness for 15 minutes, vomiting 2-3 times, bleeding from nose and pain in occipital region. At the time of admission she was conscious and oriented. There were no focal neurological deficits except anosmia. On local examination she had swelling and tenderness in the occipital region. CT scan done about 8 hours after injury showed patchy contusion involving left frontal lobe and mild cerebral oedema without any mass effect or midline shift. It also showed fracture involving posterior rim of foramen magnum. There were no other fractures or cervical spine injury. She was started on antioedma measures and prophylactic anti-convulsants. She was doing well for next two days when she became progressively drowsy and developed urinary incontinence. Immediate repeat CT scan was performed and it showed significant increase in the size of left frontal contusion with mass effect and midline shift (Figure-1). She underwent left frontal craniotomy in emergency and conservative decompression of contusion. Next day when she regained consciousness she was complaining of vision loss in left eye. On examination she had only perception of light in left eye and in right eye visual acuity was 6/24. Fundus examination showed pallor of disc in left eye and papilloedema in right eye. She also had afferent pupillary defect in left eye. Anterior segment was normal. She was started on systemic steroids, anti-oedema measures were continued. After two weeks she was further investigated with MRI and it showed signal changes in intracranial pre-chiasmatic part of left optic nerve, obliteration of surrounding subarachnoid space and swelling of the left optic nerve. Mass effect and midline shift was subsided and there were no other lesions. Follow up fundus examination showed resolution of papilloedema in right eye and minimal improvement in vision in left eye to finger counting. DISCUSSION Patients with vision loss associated with intracranial haematomas typically present with homonymous hemianopias secondary to compression of the posterior cerebral artery leading to occipital infarction during transtentorial herniation (3). This case illustrates a rarely reported phenomenon of anterior pathway vision loss involving the prechiasmatic portion of optic nerve secondary to frontal contusion without any evidence of occipital lobe injury or radiographic signs of orbit injury. The precise mechanism of anterior pathway vision loss secondary to intracranial haematomas remains poorly understood (2,3). The anterior visual pathway can be compromised directly by herniation of gyrus rectus into the suprasellar cistern, a mechanism associated with meningiomas (4). In another report it is described that intracranial optic nerve infarction can occur due to direct compression of the nerve against basal skull structures, although this specific radiographic finding was not described (2). In present case prechiasmatic optic nerve got injured probably by first mechanism leading to visual loss. This is supported by the fact that she did not have visual loss before neurological deterioration and first pre-operative CT scan did not show any mass effect, midline shift or orbital fracture. We presume that massively enlarged frontal contusion resulted in herniation of gyrus rectus into the suprasellar cistern and was responsible for compression and ischemia of optic nerve. This became clinically evident only when she regained consciousness after decompression. Post-operative MRI also confirmed the swelling of optic nerve and obliteration of the subarachnoid space on the affected side. Presence of some vision and patent subarachnoid space in the intra-orbital part of optic nerve on MRI suggested incomplete injury and partial obstruction. Also this is a rare case of post-traumatic Foster-Kennedy syndrome. Foster-Kennedy syndrome is characterized by a triad of ipsilateral optic atrophy, contralateral papilloedema and ipsilateral anosmia (5). Present case also supports the original hypothesis of Foster-Kennedy that ipsilateral optic atrophy results from direct pressure on the optic nerve, and the contralateral disc edema is ‘the result of generally raised intracranial pressure’ (5). However anosmia may be secondary to trauma in this patient. Though increasing availability of computed tomographic scanning has changed the management of head injury patients. Still rapidly enlarging intracranial haematomas can affect vision through compression or vascular compromise at many points along the visual pathway. With limited resources particularly in developing countries it may not be feasible to perform serial CT scans to monitor the size of haematomas. In these settings clinical parameters decide the timing of imaging and subsequent need for surgical intervention. However in present case it was difficult to interpret at what point of time and how much decompression of dominant frontal lobe would had prevented injury to optic nerve. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07010f2.jpg] [gm07010f1.jpg] |
| |||||||||

{kind=link}