 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
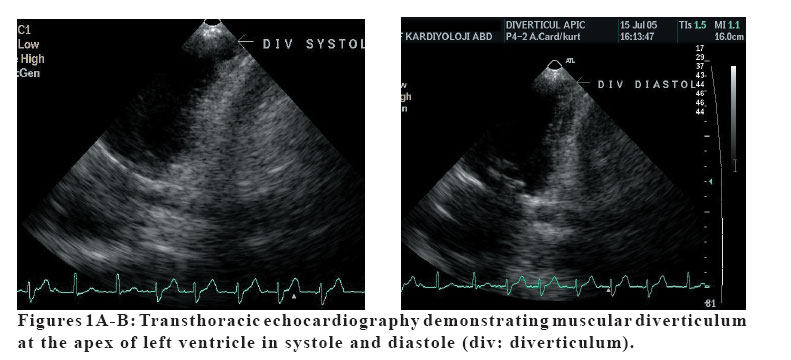
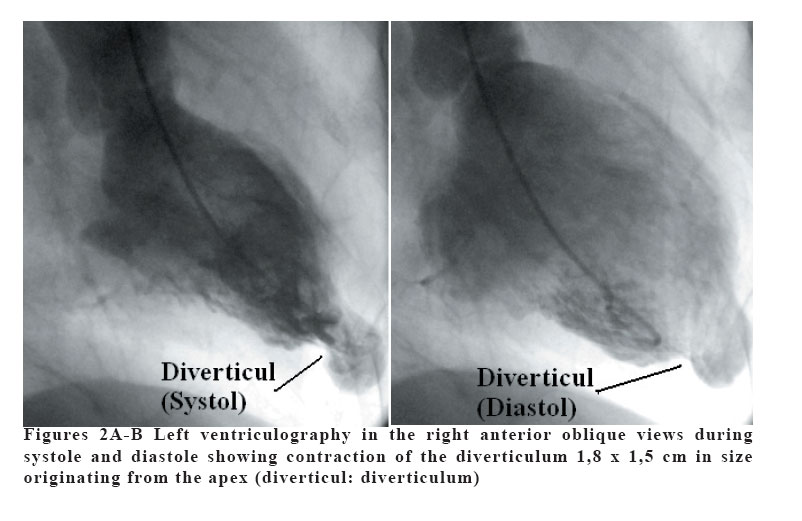
European Journal of General Medicine, Vol. 4, No. 1, 2007, pp. 47-49 AN ASYMPTOMATIC LEFT VENTRICULAR DIVERTICULUM Mehmet Yazıcı, Kurtuluş Özdemir, Bülent Behlül Altunkeser, Mehmet Kayrak, Sıddık Ülgen Selçuk University, Meram Medical Faculty, Department of Cardiology, Konya, Turkey Code Number: gm07011 Congenital ventricular diverticulum is defined as a protrusion of the free wall of the ventricle, including endocardium, myocardium and pericardium. They have been classified in fibrous and muscular types. Congenital ventricular diverticulum may be asymptomatic or may be present with various clinical symptoms. Diverticulum is commonly seen in childhood, and fibrous type being the most common type. Muscular type is very rare seen in adults. We report here, a case with muscular type asymptomatic congenital left ventricular diverticulum in a 65 year-old female. Key words: Left ventricular diverticulum, Echocardiography, Angiography INTRODUCTION Congenital ventricular diverticulum is defined as a protrusion of the free wall of the ventricle, including endocardium, myocardium and pericardium. A weakness of the myocardial wall during the embryogenesis may cause a focal protrusion of the ventricular wall (1). Congenital ventricular diverticulae have been classified in fibrous and muscular types (2). The fibrous type localized either in the apical or subvalvular area, exhibits a narrow neck, and often leads to mitral and aortic regurgitation (3). Muscular diverticulae are most often localized at the apex part of the inferior or anterior walls of the left ventricle (4). They are most commonly diagnosed in the early childhood period because of their frequent association with other cardiac and midline thoraco-abdominal anomalies; such as ventricular septal defect, tricuspid atresia, and tetralogy of Fallot (5). Diverticulum is very rare especially in adults. The incidence was reported to be about 0.4 percent in an autopsy series of adult patients with cardiac death (6). They may be asymptomatic or may present with systemic embolization, heart failure, valvular regurgitation, ventricular disrhythmia, rupture and sudden death (7,8). We report a case of left ventricular diverticulum in a patient with valvular heart disease and atrial fibrillation. CASE A 65 year-old female patient was referred to our clinic with the complaints of progressive dyspnea and palpitation. She had a history of valvular heart disease and hypertension since 1986. Physical examination revealed a normal body habitus. Vital signs were normal. Heart rate was 110 beats/min with irregular heart rhythm, and blood pressure was 140/70 mmHg. A systolic apical murmur was heard, indicating the possibility of mitral regurgitation. Pulmonary and abdominal examination was unremarkable. The 12-lead electrocardiogram showed atrial fibrillation with rapid ventricular response. Echocardiographic examination showed mild mitral regurgitation, pulmonary hypertension (40 mmHg), and contractile muscular diverticulum at the apex of left ventricle (Fig. IA-IB). Coronary angiogram was performed, which showed normal coronary arteries. Left ventriculography in the right anterior oblique view revealed an isolated contractile diverticulum 1,8 x 1,5 cm in size originating from the apex (Fig. IIA-IB). Left ventriculography also revealed mild mitral regurgitation. DISCUSSION In child, ventricular diverticulum has been commonly observed as muscular type (9), the majority of ventricular diverticulum in adults have been classified as fibrous type (4). The fibrous type is localized near the atrioventricular valve ring. It is never associated with midline defects or congenitally cardiac malformations. As in our case, muscular diverticulae are usually localized at the apex, mostly involving the inferior or anterior walls of the left ventricle, and frequently associated with thoraco-abdominal defects known as Cantrel syndrome (1,2,7). Diverticulum can be diagnosed by ventriculography, magnetic resonance imaging and 2-D echocardiography. However, standart 2-D echocardiography may not detect some diverticulae. In this situation intersectional 2-D echocardiographic views may be useful. Diverticulum is often difficult to distinguish from aneurysm. As seen in our case, the wall of diverticulum is formed by endocardium, myocardium and pericardium, and contracts normally, whereas an aneurysm is a fibrous saccular lesion and contracts paradoxically (1,8). As in our case, many cardiac diverticulae are clinically silent, but they can cause ventricular disrhythmia, systemic embolisms, or ventricular rupture and sudden death (10,11). The prognosis of isolated, asymptomatic left ventricular diverticulum is unknown. In a symptomatic patient with left ventricular diverticulum or in a patient in whom diverticulum is associated with other cardiac anomalies, surgical treatment has generally been advised. It is controversial whether an asymptomatic patient with isolated left ventricular diverticulum needs an operation. Although some authors have suggested that surgical therapy has to be advocated, others argued that surgical therapy has greater risk due to post operative complications (5-7). We did not recommend surgery to our patient since she was asymptomatic and uncomplicated with other lesions. She is under follow-up and well at the present time. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07011f1.jpg] [gm07011f2.jpg] |
| |||||||||

{kind=link}
{kind=link}