 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
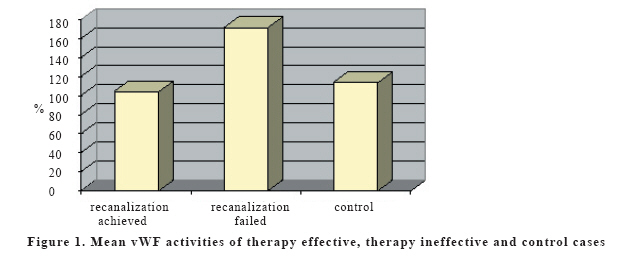
European Journal of General Medicine, Vol. 4, No. 2, 2007, pp. 57-61 RELATIONSHIP BETWEEN VON WILLEBRAND FACTOR ACTIVITY AND THERAPEUTIC SUCCESS OF THROMBOLYTIC THERAPY IN PATIENTS WITH MYOCARDIAL INFARCTION İlhami Kiki1, Nuri Köse2, Mehmet Gündoğdu1, Hasan Kaya3, Ramazan Çetinkaya1 Ataturk University School of Medicine Departments of Internal Medicine1 and Cardiology2, Erzurum, Mustafa Kemal University Medical Faculty Department of Internal Medicine3 Hatay, Turkey Correspondence: Dr. İlhami Kiki. Atatürk Üniversitesi Tıp Fakültesi İç Hastalıkları AD 25240-Erzurum/Turkey Tel: 904422361212-2106,GSM: 05324859000. Fax: 904422361301 E-mail: kikiilhami@yahoo.com Code Number: gm07015 Aim: Von Willebrand Factor is a glycoprotein, which plays role in primary hemostasis, mainly acts getting platelets to adhere onto the subendothelial tissue and carrying Factor VIII. Although vWF deficient animals had been shown to be resistant to atherosclerosis and thrombotic events, it had not been proven in humans. In this study, we aimed to investigate whether a relationship exists between VWF activity and therapeutic success of thrombolysis. Key words: Von Willebrand Factor, myocardial infarction, thrombolytic therapy. INTRODUCTION Von Willebrand Factor (VWF) is a multimeric glycoprotein molecule, which plays a central role in primary haemostasis mainly having platelets adhere onto the subendothelium. VWF also carries Factor VIII (FVIII) and prolongs its half life in the plasma. It is produced in endothelial cells and megakaryocytes (1). The most common cause of acute myocardial infraction (AMI) is intra-arterial thrombosis as a result of an atherosclerotic plaque rupture, which is including large amount of tissue factor. Several agonists such as collagen, epinephrine, ADP and serotonin promote platelet aggregation. Another important factor that participates in the pathogenesis of this event is vWF which initiates platelet adhesion by interacting with Glycoprotein Ib (GPIb) receptors and promotes aggregation by binding activated Glycoprotein IIb/IIIa receptors together with fibrinogen. The most important therapeutic approach for reducing morbidity and mortality is early thrombolytic therapy due to the existence of direct association between the amount of ischemic and necrotic tissue and morbidity and mortality rate (2). It has been reported that pigs with von Willebrand disease (vWd) are resistant to atherosclerosis, but in an autopsy study, it was reported that vWd did not protect against the development of atherosclerosis in humans, although any sign of arterial thrombosis had not been found (3,4). In this study we aimed to determine whether a relationship exists between pre-treatment vWF activity and the success rate of thrombolytic therapy in patients with myocardial infarction. MATERIALS AND METHODS Forty cases who referred to Department of Cardiology between February 2002 - June 2003 due to AMI and thrombolytic therapy been administered within 6 hour of post myocardial period were included in this study. Thirty age and sex compatible healthy controls were accepted as a control group. Blood samples of the cases were taken via forearm vein prior to the administration of thrombolytic therapy and collected in sodium citrate containing tubes. All samples were immediately centrifuged for 15 minutes at 3000 rpm and plasma was separated. Control samples were collected by the same procedure. Plasma samples of the cases and controls were stored at −80°C until they were analyzed for vWF activity. After obtaining of plasma samples, thrombolytic therapy was instituted in all cases by tissue plasminogen activator (tPA) according to standardized thrombolytic therapy procedure. Patients who determined TIMI grade 2 and 3 by angiography and/or ST segment resolution of 50% or greater, the appearance of reperfusion arrhythmias and the resolution of chest pain were accepted as successful myocardial reperfusion (5). At the time of analysis, all samples were taken out from the freezer and dissolved in 37oC water bath. VWF activity for each sample was measured by Diagnostica Stago kit (STA Compac). Plasma vWF activity of the 24 cases that were successfully recanalized by thrombolytic therapy was compared with those of 16 cases with failed therapy and 30 healthy control groups. Statistical analysis All statistical comparisons were performed using SPSS 11.5 for Windows. Results were shown as mean ± SD. Comparisons between patient and control groups with regard to the age and baseline vWF activity were performed using the student’s t- test. Comparisons between thrombolytic therapies succeed and failed groups were performed using the non-parametric Mann-Whitney U test. RESULTS Mean ages of 40 patients with AMI and 30 healthy controls were 56.0±13.0 (26-78) and 54.4±9.1 (39-71) respectively (p>0.05). Mean vWF activities of patient and control groups were 131.0±64.0 (38-254) and 113.9±47.7% (44-211) respectively (p>0.05). Coronary arterial recanalization was achieved in 24 of 40 patients (60%). Mean ages of recanalization achieved and failed patients were 53.0±4.9 (26-78) and 60.5±8.1 (47-72) respectively (p>0.05). By comparing therapy effective and ineffective cases; average vWF activity was 103.9±58.9% (38-213) in recanalization achieved patients whereas 171.7±49.0% (92-254) in therapy failed ones. Thrombolytic therapy ineffective cases had significantly higher mean vWF values than both therapy effective and control ones (p<0.01 and p<0.01 respectively). Results were shown in Figure 1. DISCUSSION In this study we have investigated the activity of vWF in patients with MI and predictive value of its pretreatment levels to estimate fibrinolytic therapy outcome. Von Willebrand Factor is a multimeric molecule, which is existed in the sub endothelium, Weibel-Palade bodies of endothelial cells, alpha granules of platelets and plasma. Basically it is formed by 275 KD monomers tied each to other by disulfide bonds. It participates in thrombus formation by means of binding to glycoprotein Ib (GPIb) adhesion receptors especially in case of endothelial injury due to high shear stress condition (1). Several studies had been performed to reveal if vWF takes part in the pathogenesis of various thrombotic events in addition to its role of primary hemostasis. There are a number of reports concerning with the association between increased vWF activity, decreased vWF cleavage (ADAMTS-13) and various thrombotic events such as myocardial infarction, thrombotic thrombocytopenic purpura and stroke. (7-11). In our study, although mean vWF activity was higher in patients with MI than healthy controls, difference was not statistically significant. This may be due to the small number of cases. Early coronary reperfusion is main therapeutic approach in current treatment of MI. Fibrinolytic therapy can reduce the relative risk of hospital death by up to 50% when administered within the first hour of the onset of symptoms. This therapy reduces infarct size, limits left ventricle dysfunction and decrease the incidence of serious complications such as septal rupture, cardiogenic shock and malignant ventricular arrhythmias (2). It had also been shown that early coronary reperfusion might blunt the early post infarction procoagulant state by reducing the response to plasminogen activator inhibitor and vWF activity, prevent inflammation and thromboembolic complications, increase the plaque stabilization and reduce morbidity and mortality, (9-11). In our cases, thrombolytic therapy has been administered within first six hour of MI. It is widely accepted that the earlier therapy is related to better outcome. However fibrinolytic therapy remains of benefit for many patients seen 3 to 6 hours after the onset of infarction (1). In our study we have found that patients with MI and high levels of vWF activities, had significantly less benefit from the fibrinolytic therapy and vice versa. However these results reflect acute effect of thrombolytic therapy. Further studies are needed to determine the long terme results in both groups. It can be hypothesized that a successful thrombolytic therapy might break the vicious circle of the uncontrolled coagulation by reducing the levels of vWF and other procoagulant factors and lead to increase in the recanalization rate. As a matter of fact, both vWF and fibrinogen levels that measured immediately after angioplasty were shown that independent predictors for restenosis (15). It was also demonstrated that high levels of vWF in early period of unstable angina pectoris was associated with worse prognosis such as development of myocardial infarction, recurrent anginal attacks and delayed revascularization (16). Von Willebrand Factor levels were found high not only in thromboembolic events but also in certain conditions constituting risk factors for thrombosis such as obesity and older age suggesting that vWF may at least partly responsible for thrombotic events, which are seen frequently in such people (17, 18). If possible role of vWF in vascular thrombosis is considered, it can be thought that prognosis of such events might be improved by blockade of its effect. Several animal studies showed that blocking of vWF and platelet GPIb receptor interaction by using aurintricarboxylic acid (ATA) significantly reduced rate of restenosis in the vessels which are recanalized by tPA. In these studies ATA was also shown that inhibits neointimal lesion formation and smooth muscle proliferation (19-22). These results bring to mind the important role of vWF in the pathogenesis of reocclusion and restenosis developing after thrombolytic therapy. As a conclusion; in this study we found that vWF activity is significantly lower in controls and patients who successfully recanalized by thrombolytic therapy than therapy failed ones. In addition to being an independent risk factor for coronary heart disease, higher levels of vWF activity in thrombolytic therapy failed patients, might suggest the predictive value of this factor to estimate the therapeutic success of thrombolysis REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07015f1.jpg] |
| |||||||||

{kind=link}