 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
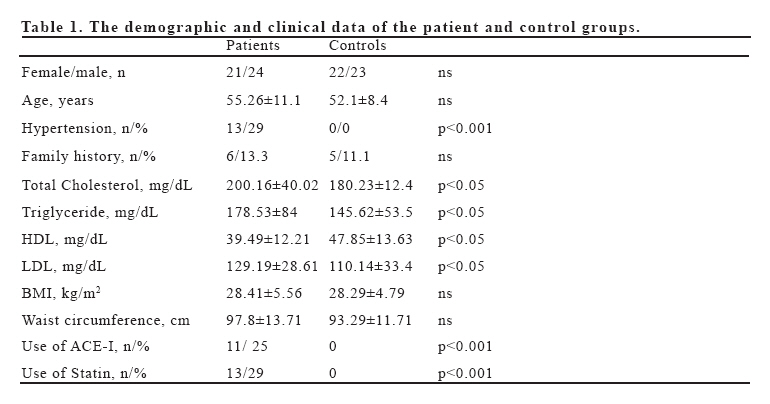
European Journal of General Medicine, Vol. 4, No. 2, 2007, pp. 62-66 THE RELATIONSHIP BETWEEN OXIDATIVE STRESS, NITRIC OXIDE, AND CORONARY ARTERY DISEASE Serdar Soydinç1, Ahmet Çelik2, Seniz Demiryürek3, Vedat Davutoğlu1, Mehmet Tarakçıoğlu2, Mehmet Aksoy1 University of Gaziantep, School of Medicine, Departments of Cardiology1 and Biochemistry2, Gaziantep, Gazi University, Faculty of Medicine,Department of Physiology3, Ankara, Turkey Correspondence: Ahmet Celik. Gaziantep University, Department of Biochemistry, Faculty of Medicine, 27310 Gaziantep, Turkey Phone: 903423606060, Fax: 903423603928 E- mail: drahmetcelik@gmail.com Code Number: gm07016 Aim: Oxidative stress and free radicals are known to have important roles in the development of atherosclerosis. Malondialdehyde (MDA), a carbonile group produced during lipid peroxidation, is used widely in determining oxidative stress. Nitric Oxide (NO) is a vasodilatator agent derived from the endothelium. The aim of our study was to investigate the relationship between MDA and NO in patient with coronary artery disease. Key words: Coronary artery disease, malondialdehyde, nitric oxide, oxidative stress INTRODUCTION Oxidative stress and free radicals are known to have important roles in the development of atherosclerosis (1). Oxidative modification of LDL by free radicals results in negative effects on vascular function such as decrease in nitric oxide (NO) levels, endothelial apoptosis, increase in smooh muscle cell proliferation, and synthesis of proinflammatory molecules (2). Malondialdehyde (MDA), a carbonile group produced during lipid peroxidation, is used widely in determining oxidative stress. NO is a vasodilatator agent derived from the endothelium, which is synthesized by the NO synthetase and converted into its more stable forms nitrite (NO2) and nitrate (NO3) in plasma. Besides regulating blood pressure through its main effect i.e. vasodilatation, it also has inhibitory role in thrombocyte aggregation, leukocyte adhesion, smooth muscle cell proliferation and LDL oxidation. The decrease in synthesis and bioavailability is an important step in the development of atherosclerosis (3). The aim of our study was to investigate the relationship between coronary artery disease (CAD), oxidative stress and NO. MATERIAL AND METHODS Subjects Forty-five patients diagnosed with 50 % or more stenosis by coronary angiography were included in our study. Patients were separated as 1, 2 and 3 vessel-patients according to the number of vessels affected. Diabetics, smoking patients, patients with malignancy, renal and liver disease, and patients using nitrate preparation were excluded from the study. Forty-five healthy individuals, who had cardiological evaluation in the last year, had no history of diabetes, dyslipidemia, smoking, heart disease, or cancer were identified as the control group. Blood Samples Blood samples were obtained from the antecubital veins in all subjects, following a 12-hour fast and kept at –80 oC until the time of analysis. Measurement of Serum Lipids Serum total cholesterol, triglyceride and HDL levels were measured with enzymatic-colorimetric method in biochemistry auto-analyzer using the Roche commercial kit. Serum LDL levels were calculated according to the Friedewald formula (4). Measurement of Serum NO Ethanol with abso cooled at a rate of 1:2 v/v (00C) was added to the serum samples, which were then vortexed and deproteinized. Samples were centrifuged for 5 minutes at 14 000 rpm, following a 30-minute incubation at 0oC. The supernatant was used for the measurement of NO. Vanadium (III)–HCl (reducing agent) at 95oC was injected into the supernatant and the measurement of NO, produced as a result of the reduction of nitrate, nitrite and S-nitroso compounds, was performed using the analyzer NOA 280 (Sievers Instruments, Boulder, CO, A.B.D.) with the NO/ozone chemiluminescence technique. All samples were studied twice. The standard curve was formed using dilutions of NaNO3 (0.1-100 µM). Concentrations of the NO metabolites in the samples were determined using the standard curve and the serum samples were calculated as µM. The NOAnalysisTM (version 3.21, Sievers, Boulder, CO, A.B.D.) program was used for the measurements and analyses. Measurement of Serum MDA Lipid peroxidation was estimated by measurement of thiobarbituric acid reactive substances (TBARS) in serum by the method previously described by Draper et al (5). After the reaction of MDA with thiobarbituric acid, the reaction product was followed spectrophotometrically at 532 nm, using tetrametoxypropane as a standard. The results are expressed as nmol/ml. Statistical Analysis Statistical analyses of the data obtained in the study were done using the SPSS (Statistical Package for Social Sciences) for Windows 10.0 program. Quantitative values of the groups are given as the mean ± standard deviation, whereas qualitative values are given in percentages. “One-way ANOVA”, “student’s t-test” and “Kruskal-Wallis test” was used for the evaluation of the differences between the main groups. “Mann-Whitney U test” was used for the biological markers of CHD and for each variable. P < 0.05 value was accepted significant in all of the results. RESULTS The demographic and clinical data of the patient and control groups are presented in Table 1. There were no significant differences between the groups in terms of age, sex, body mass index, and waist circumference. In the coronary artery disease (CAD) group, total cholesterol, LDL cholesterol and triglyceride levels were significantly higher in comparison to the control group; whereas HDL cholesterol levels were lower (p< 0.05). Serum MDA levels were significantly higher in the patients when compared to the control group (3.97 ± 1.21 vs. 2.91 ± 0.84, respectively p<0.001). No statistical differences were determined in the comparison of the spread of coronary artery disease and MDA levels. When NO levels were compared in the patient and control groups, NO was tended to be higher in the patients (38.43±19.74) than the controls (35.19±29.35) (p>0.05). No significant differences were determined in the comparison of NO levels between one, two and three vessel patients. NO levels were significantly higher in hypertensive CAD patients than the normotensive ones (p<0.05). There was a significant relation between NO levels and body mass index in subjects with CAD. While NO was 48.6±13.7 in patients with BMI above 25, it was found to be 33.5±18.2 in patients with BMI below 25 (p<0.01). DISCUSSION In the present study, MDA levels as a marker of oxidative stress showed highly significant relation with coronary artery disease revealing the interrelation between the oxidative stress and the atherosclerosis. We found this relationship independent from the NO levels which were mildly increased in the patient group. This study added more proof about the oxidative stress and the coronary artery disease. The role of oxidative stress in the development of coronary artery disease is well known. The MDA, a carbonile group produced during lipid peroxidation, is used widely in determining oxidative stress. Increased MDA levels in coronary artery disease were demonstrated in several clinical studies. In our study we demonstrate firstly this effect as an independent phenomenon from the NO level. Mendis et al. showed that in acute coronary syndromes and stable angina pectoris, which reflect the acute and chronic forms of the disease, serum total MDA was higher than those of the controls (6). Kostner et al. reported high MDA levels in coronary artery patients (7). Pucheu et al. reported an increase in serum MDA following thrombolysis in patients with acute MI, although they could find no significant differences between patients with stable angina pectoris and the control group (8). In a study of Cavalca et al. in which serum free and total MDAs were measured synchronously, significantly higher MDA levels were determined in coronary artery patients in comparison to the control group (9). In our MDA study, we found higher MDA levels of high statistical significance in the group with coronary artery disease when compared to the control group. Although we thought that MDA might also be related with coronary involvement, we did not determine any relationship between these two parameters. Besides being an endothelium derived vasodilatator molecule, NO also has important physiological and pathological effects. It can be synthesized in most tissue and cells. Its most prominent roles in cardiovascular system are blood pressure regulation, inhibition of thrombocyte aggregation, leukocyte adhesion, smooth muscle cell proliferation, and LDL oxidation. The decreases in production and bioavailability are associated with events that accelerate development of atherosclerosis such as vasoconstriction, thrombocyte aggregation, migration of monocytes to the vascular wall, oxidized LDL and foam cell production. The main hypothesis of our study was that increased oxidative stress could reduce NO synthesis. Although patients with CAD had increased MDA levels, no significant correlations were determined between MDA and NO. NO levels were tended to be higher than those of the control group. NO levels showed a significant relation with higher BMI and hypertension in coronary artery disease. It was suggested that adipose tissue contains NO synthetase enzyme, and is thus a potential NO source (10,11). In a study performed with healthy individuals at adolescent age, it was demonstrated that serum NO levels highly correlated with BMI and that NO levels were significantly higher in obese individuals. In our study, serum NO levels were found significantly higher in patients with BMI>25 kg/m2 (p<0.05). There are evidence indicating increased NO levels in hypertensive patients (12). Compensatory mechanisms against high blood pressure increase NO secretion from the vascular endothelium. NO levels of hypertensive subjects were significantly higher than those of the normotensives in our patient group (p<0.05). Similar results were also obtained in the study of Yoon et al. performed on coronary artery patients (13). In the study, NO levels were statistically significantly higher in coronary artery patients with hypertension when compared to those without hypertension. Again in the same study, NO levels of the coronary artery patients without hypertension were similar to those of the control group. An important portion of the hypertensive patients included in our study was receiving ACE inhibitors. In our opinion, other than the effects of compensatory mechanisms, which developed secondary to hypertension, the ACE inhibitors used in our hypertensive group also contributed to the high NO levels. The rapidly increasing data indicating a positive effect of ACE inhibitors on endothelial function, suggest that serum NO levels might increase as an evidence of improved endothelial function (14). Although the hypothesis of our study was that decreased NO levels could be observed in response to increased oxidative stress in coronary artery patients, our results revealed NO levels similar to those of the control group. There are studies, which show that serum NO levels are decreased or not changed in coronary artery patients (15,16). However, no study was found among all studies which could identify the exact relation of serum NO levels with coronary artery disease. We think that the different data on the relationship between NO and CAD are due to the fact that serum NO levels might be affected from several parameters and that although endothelial dysfunction has developed, normal serum NO levels might still be observed. Therefore, we think that it is more appropriate to directly evaluate endothelial function through methods such as acetylcholine, FMD, rather than serum NO levels, in determining endothelial dysfunction leading to atherosclerosis or atherosclerotic disease. In conclusion, we found more proof about relationship between oxidative stress and coronary artery disease. MDA levels as a marker of oxidative stress showed highly significant relation with CAD as an independent effect from NO level. MDA and NO showed no significant interrelation. The high MDA levels among all patients with CAD demonstrate a relationship between the oxidative stress and the atheroslerosis. The role of the antioxidant treatment in coronary heart disease need to be determined. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07016t1.jpg] |
| |||||||||

{kind=link}