 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
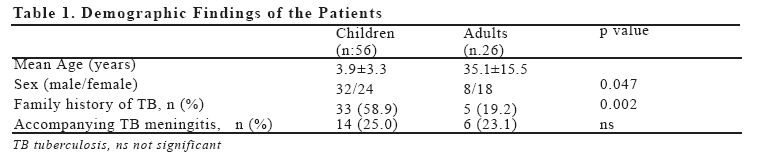
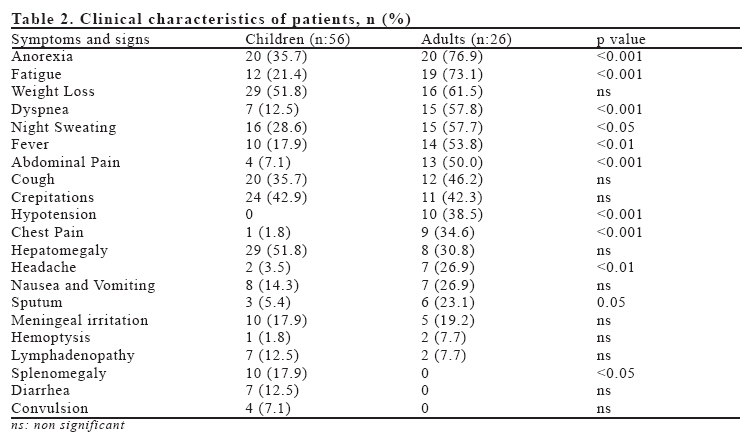
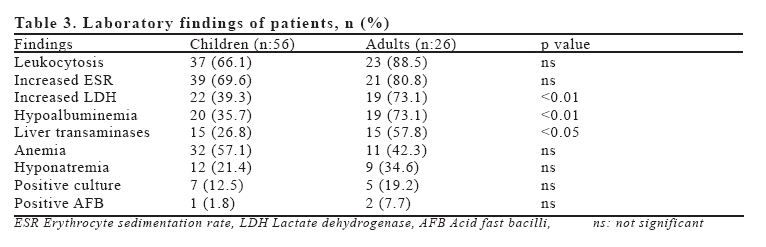
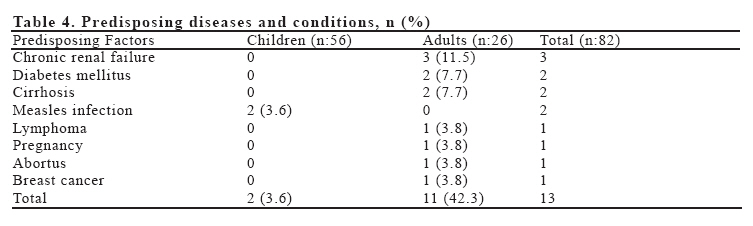
European Journal of General Medicine, Vol. 4, No. 2, 2007, pp. 67-72 A COMPARATIVE REVIEW OF PEDIATRIC AND ADULT PATIENTS WITH MILIARY TUBERCULOSIS Çetin Tanrıkulu1, Fuat Gürkan2, Canan Eren Dağlı1, Ayfer Gözü2, Ali Süner3 Dicle University Medical Faculty, Departments of Chest Diseases1, Pediatrics2 and Internal Medicine3, Diyarbakir, Turkey Correspondence: Dr. Fuat Gürkan, Dicle University Medical Faculty, Department of Pediatrics, Diyarbakir, Turkey. Tel: 904122488001/4395, Fax: 904122488074 E-mail: fgurkan@dicle.edu.tr, fuatgurkan@hotmail.com Code Number: gm07017 Aim: Miliary tuberculosis (MTB) is a serious and rare form of tuberculosis. Studies comparatively reviewed children and adults with MTB are lacking. Key words: Miliary tuberculosis, diagnosis, clinical characteristics, adult, child INTRODUCTION Approximately one-third of the world’s population (1.7 billion people) is infected with the tuberculous (TB) bacilli (1). Due to advent of HIV/AIDS and the resurgence of TB, global attention has been focused on adult forms of TB, and there is a real danger that TB in children may be overlooked. In clinical experience, the signs and symptoms of TB in children are so vague that diagnosis is often difficult. On the other hand, missed diagnosis of TB is as common as over diagnosis in childhood (1). Miliary tuberculosis (MTB) results from the acute hematogenous dissemination of TB bacilli in lungs and other organs, where numerous small tuberculous granulomas develop. Although classically seen in children, there is increasing incidence of MTB in adults and elderly subjects (2). The disease consists 3-7% of all forms of tuberculosis infections, and the mortality rate may be high particularly in children reaching up to 25% (1). Diagnosis may sometimes be delayed, since the positivity of acid fast bacilli (AFB) on the sputum smear is only found in one-third of the cases, probably because of the propensity of pediatric cases. There is concern regarding increasing rates of TB and MTB among patients with HIV infection (3-9). Diagnosis of MTB may be more difficult in a non-HIV area. The aim of this study was to investigate the clinical, radiological and laboratory characteristics, outcome and risk factors of pediatric and adult patients with MTB in a comperative manner at a non-HIV area in order to obtain an early diagnosis and treatment of MTB. MATERIALS AND METHODS The records of MTB patients, both children and adults, diagnosed and treated in Dicle University Hospital between 1990 and 2003 were reviewed. Dicle University Hospital is a tertiary care center in the South East of Turkey, to which patients from all over the region are referred for diagnosis and treatment. The demographical characteristics, presenting symptoms, clinical and laboratory features, predisposing factors, treatment regimens, complications, prognosis and outcome were recorded. The diagnosis of MTB was based on the presence of miliary pattern on chest radiograph and/or typical findings on high resolution computerized tomography (HRCT), along with one or more of the following features: 1) clinical features compatible with tuberculosis, 2) positive smear or culture for Mycobacterium tuberculosis, 3) histopathological evidence of TB. The patients with suspicion of meningitis underwent lumbar puncture and cerebrospinal fluid was examined. Tuberculous meningitis was diagnosed according to clinical, cerebrospinal fluid, CT scan or MRI criteria. Complete blood count, serum biochemistry and Mantoux tests were performed. Blood and other specimens (gastric aspirate, sputum, and cerebrospinal fluid) were investigated for M. tuberculosis by culture and smears. Lowenstein-Jensen and/or Bac-Tec medium was used for cultures. Five tuberculin units (TU) test solution was used for Mantoux testing at diagnosis in all pediatric cases and indurations were measured after 72 hours. Mantoux testing was considered positive when indurations were larger than 10 mm and 15 mm in children without and with BCG vaccination, respectively. All patients were treated with isoniazide (INH) (15mg/kg/day, maximum 300mg/day), and rifampisin (15mg/kg/day, maximum 600mg/day) for nine to twelve months and additional pyrazinamide (30mg/kg/day, maximum 2gr/day) and ethambutol (20mg/kg/day, maximum 1.5gr/day) or streptomycin (30mg/kg/day, maximum 1gr/day) for the first two months period. All cases were called for periodic controls every month during the whole treatment period. Statistical analysis was performed using Chi-square test and Student’s t test for comparison between children and adults. P values less than 0.05 were considered significant. RESULTS A total of 82 patients were included (37 male and 45 female), 26 were adults and 56 were children (<15 yrs). The mean age of the pediatric patients was 3.9±3.3 years (range, 0.6-14) and the adults was 35.1±15.5 years (range, 19-65). There was a male predominance in pediatric and female predominance in adult patients (p<0.05) (Table 1). Thirty-eight (46%) of all patients of whom 33 were children had family history of tuberculosis. None of the patients had prior history of tuberculosis in the past. The percent of accompanying TB meningitis were similar in children (25.0%) and adults (23.1%) with MTB (p>0.05) (Table 1). Adults had more commonly symptoms and signs of anorexia, fatigue, dyspnea, night sweating, fever, abdominal pain, hypotension, chest pain and headache than the child patients (P<0.05). The most frequent symptoms and signs of children were weight loss, hepatomegaly, crepitations, anorexia and cough (Table 2). Hepatosplenomegaly, lymphadenopathy, diarrhea and convulsion were more common in children than in adults; however only for splenomegaly this difference reached to a marginal significant level (p<0.05) (Table 2). Hemoptysis was only seen in 1 child and 2 adults. Among all patients, the most common laboratory abnormalities were leukocytosis, increased erythrocyte sedimentation rate (ESR), increased lactate dehydrogenase (LDH), hypoalbuminemia, elevated liver transaminases and anemia (Table 3). Hypoalbuminemia, elevated levels of liver transaminases and lactate dehydrogenase were more common among adults than in children (Table 2). Microbiologically proven diagnosis was established in 15 (18.3%) patients of whom 3 had AFB positivity on sputum smear and 12 had Mycobacterium tuberculosis isolation from various cultures (1 urine culture,1 cerebrospinal fluid culture, 1 gastric fluid culture and 9 sputum cultures). Ratios of positive culture and positive AFB results were higher in adults compared with pediatric patients, however their differences did not reach to significant levels (P>0.05) (Table 2). One of the overall isolated species had isoniazide resistance. Cervical lymph node biopsies in two patients and bone marrow biopsies in two patients revealed granulomatous inflammation of tuberculosis. All patients had miliary pattern on chest X-rays. The diagnosis was confirmed by HRCT in 23 patients (16 children, 7 adults) and 3 patients had cavitary lesions. Among 56 pediatric cases, there were 8 (14.3%) children with positive BCG scar and only 16 (28.6%) children with positive reaction to 5TU tuberculin test. A total of 13 patients, 2 children and 11 adults, had an underlying predisposing disease for the development of MTB (Table 4). These were measles infection in two children; and mainly chronic renal failure, cancer, diabetes mellitus and cirrhosis in adults (Table 4). During the course of anti-TB treatment, 28 patients received steroids and 6 patients required mechanical ventilatory support. A total of 6 (7.3%) patients (4 children, 2 adults) died during hospitalization, of whom 2 had accompanying tuberculous meningitis, 2 had prior measles infection, 1 chronic renal failure and 1 acute viral hepatitis. Chest X-rays shown complete clearence of the miliary shadows at the end of 3-4 months of follow-up in 76 patients (92.7%). DISCUSSION Tuberculosis still remains a major challenge among infectious diseases and MTB is a rare form of the disease (10). In this retrospective study we compared clinical profile, laboratory characteristics and outcome in children and adult patients with MTB. All our patients had radiological appearance of miliary pattern on chest X- ray, however a diagnosis based on miliary shadowing on chest radiography may sometimes be insufficient. In the study of Kwong et al., the sensitivity of chest radiography for MTB was found to be 59-69% and specifity 97-100% (11). The high specifity and moderate sensitivity of the chest radiography identifying MTB indicates the need to look beyond the chest radiography for confirmation of the diagnosis. Some other lung diseases, for example, pulmonary alveolar microlithiasis, may show diffuse small nodular shadowing on chest X-ray resembling miliary pattern. HRCT is recommended in the assessment of patients with suspected MTB who have normal or equivocal radiographic findings (2, 12, 13, 14). A confirmation of the disease by HRCT was required in 28.1% of our patients. All patients were additionally confirmed by compatible clinical features and response to treatment. At their follow-up, pulmonary radiographic abnormalities of our patients were improved without scarring or calcification in all our patients, except 6 who died. Resolution of pulmonary abnormalities has been reported to be achieved after three months of treatment in most cases (15). The classical miliary pattern was present in 84% of 38 patients in the study of Mert et al, in 89% of 47 patients in Al-Jahdali et al’s, in 91% of 94 patients in Hussey et al’s studies (5, 7, 14). In our region, Gurkan et al have detected miliary pattern in all of their 23 pediatric patients (8). The reason for the high frequency of diagnosis with radiographic findings in our region may be suggested that patients did not apply to a doctor until the disease has progressed or the doctors usually did not consider MTB in patients when they had a normal radiography. In our series, there was a female preponderance in adults and a male predominance in children. Several studies showed a male preponderance in patients with TB (16, 17). However, female predominance of our adult patients may simply be due to small number of patients or may be related to the existence of underlying chronic diseases, since, 7 of our 11 adult patients with underlying predisposing factors were female. Symptoms and findings in patients with MTB may display a variety. Fever, loss of weight, night sweats, cough, crepitations and hepatosplenomegaly are the most commonly seen symptoms and findings (5-8). In our study, nonspecific symptoms were more common and the more specific symptoms indicating a pulmonary infection, including dyspnea, fever, cough and crepitations were found in 42.3% to 57.8% of our total study group. Most of our adult patients had non-specific symptoms such as anorexia, fatigue and weight loss. The common presenting symptoms and signs of adult patients in our study were somewhat infrequent than those of some previously reported series (4,6,16,17). Children had more insidious clinical picture of the disease. There may even be a lower definition of nonspecific symptoms in children whose symptoms were possibly ignored or not noticed by their parents because of their low educational status. In comparison with 94 children with MTB in Hussey et al’s study, children had less frequent symptoms and signs of cough (72% and 36%), splenomegaly (54% and 17.9%) and lymphadenopathy (46% and 13%) than in our study, respectively (7). A half of our pediatric patients had weight loss and/or hepatomegaly. Weight loss may be a sign of preceding malnutrition in children. Therefore we could not differentiate whether weight loss was a predisposing factor for MTB or secondary to anorexia due to tuberculosis itself. TB is common in malnutrition; however exactly how malnutrition favors the TB development is not well known (18,19). Number of patients were not different between adults and children regarding their weight loss. A number of biochemical and hematological abnormalities are reported to occur in MTB, but their significance is controversial (6). Leukocytosis and anemia of the chronic disease are well known laboratory findings of MTB (20). In our patients anemia was present in 57.1% of children and 42.3% of adults, and leukocytosis was present in a total of 73.2% patients. Additional biochemical abnormalities were mainly reported as hyponatremia, increased alkaline phosphatese and transaminase levels, hyperbilirubinemia and hypercalcemia (4, 20, 21). In the present study, comparison between adults and children revealed more frequent -but not statistically significant- anemia in children and more frequent hypoalbuminemia and elevated levels of liver transaminases and lactate dehydrogenase in adults. Hyponatremia was observed in 34.6% of our adult patients. Sharma et al. reported hyponatremia in 70.0% of their adult patients with MTB (6), suggested being due to excessive ADH production or meningeal involvement (22). Most of our patients with hyponatremia had also TB meningitis. Nearly one third of the patients with MTB have been reported to reveal AFB in the sputum in adults (6, 7). The lower frequency of AFB detection (18.3%) may be due to predominance of pediatric patients (68.3%) in our study group. It is well known that childhood TB is generally non-cavernous and low acid load and 68.3% of our patients were children. The determinants of TB dissemination include status of host cellular immunity, mycobacterial virulence and bacil load. The rate of predisposing factors such as diabetes, renal failure, malignancy, connective tissue disease, alcoholism, hematologic diseases and mainly HIV infection accompanying MTB has been reported between 23% and 76% in previous series (4, 21, 23). Our patients neither had HIV infection nor a doctor diagnosed primary immunodeficiency. We found a predisposing factor in 2 (3.6%) children and 11 (42.3%) adults. In different series, mortality rates were reported between 7.7% and 23.9% in MTB (4, 5, 7, 21). In the study of Prout et al. this rate was even higher with 40 exitus among 62 cases (64%); and all of their 25 cases who had an associated disease had died (23). Lower mortality in our patients may be due to absence of HIV or immunosuppression, the less number of cases having an accompanying disease, effective anti TB therapy and management in a tertiary health center. Central nervous system (CNS) involvement has been reported as an independent predictor of mortality in MTB, reported to occur in 16-30% of the patients (4, 18, 24). Poor prognosis has also been reported as associated with increasing age, liver dysfunction, leukocytosis, anergy, female sex or the presence of underlying disease in different studies (4, 16, 21, 25). In our study a total of 20 patients (24.4%) had accompanying TB meningitis. Among our 6 exitus patients, 2 had accompanying tuberculous meningitis, and 4 an underlying disease. Miliary tuberculosis is generally accepted as a primary tuberculosis infection. For this reason the source of the contamination should be searched. Unfortunately the probable source can not be found every time. Berktas et al have reported in their 35 adult cases of MTB that 6 (17.1%) had contact history with TB patients similarly to our results in adult patients (19.2%) (19). Mert et al have detected no prior contact with tuberculosis patients and no family contamination in their series of 38 adult cases (5). In our study, we found family history of tuberculosis in total 38 (47.3%) patients, of whom 33 (86.8%) were children. History of prior diagnosis of tuberculosis was not present in any of our patients. Negative Mantoux test was found in 66 (80.5%) patients suggesting an impaired host cellular immunity after the disease onset. Among 56 pediatric cases, there were 8 (14.3%) children with positive BCG scar. High rate of history of family contact and low rate of BCG vaccination in our patients with MTB were significant public health problems. This low rate of BCG vaccination was found to be valuable to emphasize the role of early BCG vaccination in infancy to prevent hematogenous dissemination of TB infection in early ages at a TB prevalent area. According to our results, high clinical suspicion and efforts for early confirmation of the diagnosis are imperative, due to scarcity of disease specific symptoms and signs, especially in children. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07017t1.jpg] [gm07017t2.jpg] [gm07017t4.jpg] [gm07017t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}