 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
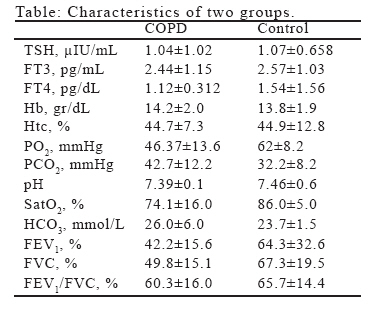
European Journal of General Medicine, Vol. 4, No. 2, 2007, pp. 80-82 THYROID HORMON LEVELS IN PATIENTS WITH ACUTE EXACERBATION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE Kürşat Uzun1, Hüseyin Atalay2, Ali İnal2 Selçuk University, Meram Medical Faculty, Pulmonary Diseases1 and Internal Medicine2, Konya, Turkey Correspondence: Dr. Kürşat Uzun. Selçuk Üniversitesi Meram Tıp Fakültesi, Göğüs Hastalıkları AD, Konya, Türkiye. Tel: 903322236397, Fax: 903323237121 E-mail: uzunkur@yahoo.com Code Number: gm07019 Aim; The severity of airway obstruction in chronic obstructive pulmonary diseases (COPD) is associated with impairment of thyroid gland function. Key words: COPD, thyroid hormones, pulmonary function tests, arterial blood gases INTRODUCTION Abnormalities in thyroid hormone regulation are encountered frequently in nonthyroidal diseases; these include normal or decreased total and free thyroxine (TT4 and FT4 respectively), decreased total (TT3) and free (FT3) triiodothyronine along with usually normal thyroid-stimulating hormone (TSH) levels (1). These changes have been observed primarily in critical illness, such as starvation, sepsis, surgery, or myocardial infarction, but also in diverse chronic, systemic conditions, i.e., in chronic heart failure, chronic liver or hematological diseases, cancer, diabetes, and in connective tissue disorders (2-4). Chronic obstructive pulmonary disease (COPD) is a major cause of chronic morbidity and mortality throughout the world, leading to years of suffering and premature death from it or its complications (5). The severity of airway obstruction in COPD is associated with impairment of thyroid gland function (6). There is an apparent clinical resemblance between a hyperthyroid state and advanced COPD. Early detection of thyroid disturbances may therefore be clinically important in COPD (4, 7). In the present study, we evaluated thyroid abnormalities in patients with COPD and relationship between pulmonary function tests, arterial blood gases and thyroid functions. MATERIAL AND MATHODS Subjects The patient group comprised of 62 COPD patients aged 64.5±8.3 (51-74) years and 20 control subjects aged 62.1±5.7 (45-68) years. The patients with COPD were diagnosed according to Global Initiative for Chronic Obstructive Lung Disease Criteria (8). All patients were ex-smokers and they were clinically in exacerbation. All patients received medicine related to COPD (inhaler/oral bronchodilators and intravenous/oral steroid, and antibiotics). The patients were not receiving iodine-containing drugs. Control groups comprised of patients without COPD. Control group included cases with lung cancer, hydatid cyst, asthma, pulmonary embolism, and pneumonia. The controls did not receive iodine, bronchodilators and steroids. Study Design The patients were admitted to the pulmonary department. In all patients, a clinical history was taken and physical examination was performed. Pulmonary function tests and arterial blood gas analysis were performed in patients with stable COPD. Serum levels of free triiodothyronine (FT3), free thyroxine (FT4) and thyroid-stimulating hormone (TSH) were determined by using the commercial IMMULITE kits, which are solid-phase, two-site chemiluminescent immunometric assays (Immullite, DPC, USA). Statistical Analysis Results were expressed as the mean±SD. Statistical analysis was performed by Student’s t test. Significance was defined as a p value <0.05. RESULTS The characteristics of all patients were showed in table. All patients with COPD suffered from severe irreversible airway obstruction with a FEV1 in percentage predicted of 42.2±15.5 %. All patients with COPD had hypoxemia (mean PaO2: 46.4±13.6 mmHg), but PaCO2 was within normal limits (mean PaCO2: 42.7±12.2 mmHg). The mean levels of TSH, FT3 and FT4 were within normal limits in two groups. There was no significant difference in mean levels of TSH, FT3 and FT4 between COPD and control group (p>0.05, p>0.05, p>0.05). Serum level of TSH was lower than normal limits in 20 of 62 patients with COPD. Serum level of FT3 was higher than normal limits in 2 of 20 patients with lower TSH level. Serum level of FT4 was in normal limits in all patients with COPD. In control group, TSH was lower than normal limits in 2 patients, but FT3 was normal in these patients. There was significant difference according to TSH and FT3 between COPD and control group (p<0.01). There was significantly positive correlation between FT3 and saturation of oxygen (p<0.05). There were negative correlations between FT4 and hemoglobin or hematocrite levels (p<0.05, p<0.05) (r: -337, r: -281, respectively). There were no correlation between TSH, FT3 or FT4 and PaO2, PaCO2 and pulmonary function tests. DISCUSSION There is an apparent clinical resemblance between a hyperthyroid state and advanced chronic obstructive pulmonary disease (COPD). In both conditions tachycardia, weight reduction and loss of muscle mass may be found. In COPD complicated by hypoxaemia these traits may be aggravated, since chronic or intermittent hypoxaemia may trigger a hypermetabolic state causing depletion of fat free mass (1). Dimopoulou et al. (9) found that all patients had normal values for resting thyroid hormones. However, in severe COPD, a certain degree of thyroid dysfunction was evident. Semple et al. (10) measured serum TT3 and TT4 levels in 16 patients with stable COPD having a mean FEV1 below 40% of predicted and did not find any difference among hypercapnics, normocapnics and controls. Gow et al. (11) investigated thyroid function in 20 patients with exacerbation, having severe COPD (highest FEV1 40% of predicted). They did not find any correlation between arterial blood gas measurement and thyroid hormone concentrations in patients with COPD. Okutan et al. (12) found that level of FT3 was higher in stable COPD than control group. They reported that there was negative correlation between pulmonary function tests and PaO2 or FT3. In our study, the mean levels of thyroid functions were normal in two groups, but there was lower TSH than normal limits in 20 patients with COPD and in 2 patients without COPD. All of our patients had severe COPD. In our study, there was significantly positive correlation between FT3 and saturation of oxygen. There were negative correlations between FT4 and hemoglobin or hematocrite. There was no correlation between thyroid hormone levels and pulmonary functions. Banks and Cooper (13) found no relationship between hormonal levels and lung function in patients with chronic lung disease, and they suggested that most of endocrine dysfunction ascribed to COPD was probably due to factors other than hypoxia or hypercapnia. We did not find any association between hormonal levels and hypercapnia or hypoxia. In other chronic conditions, such as chronic heart failure, the occurrence of thyroid dysfunction has been found to correlate with diseases severity (14). Our patients had severe COPD and exacerbation. We suggest that severe airway obstruction and excessive respiratory muscle load affect thyroid hormone levels in patients with COPD. In conclusion, the mean levels of thyroid hormones were similar in two groups. Hypoxia and hypercapnia did not correlate with thyroid hormones. We have demonstrated that both clinic and subclinic hyperthyroidism were higher in patients with COPD exacerbations than cases without COPD. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07019t1.jpg] |
| |||||||||

{kind=link}