 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
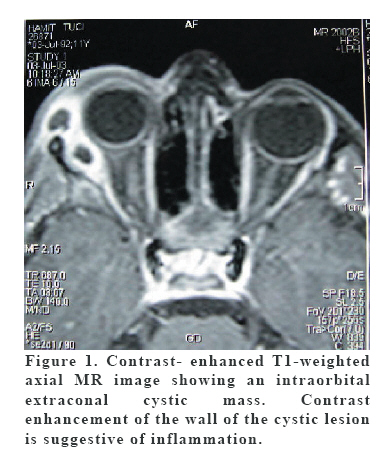
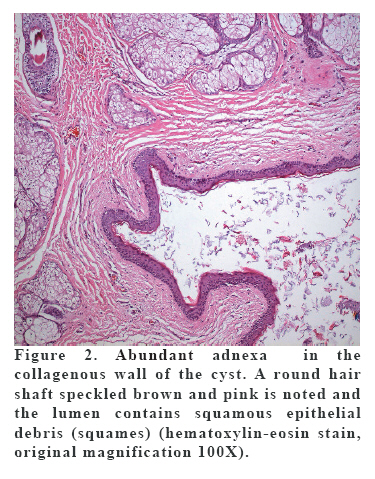
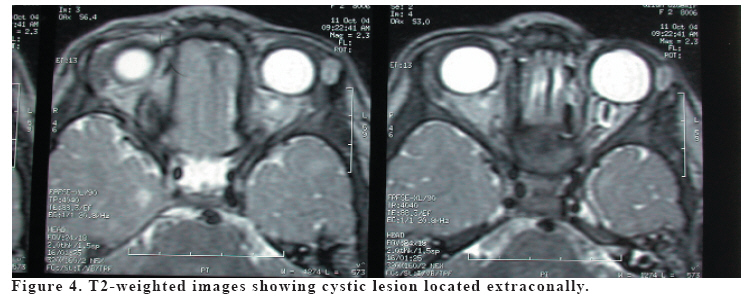
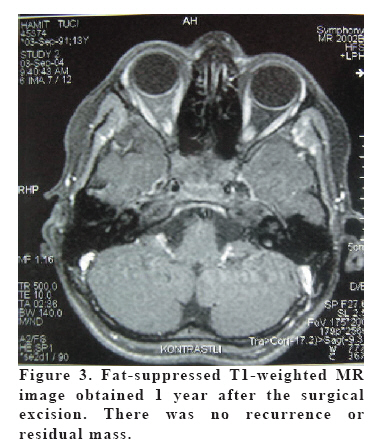
European Journal of General Medicine, Vol. 4, No. 2, 2007, pp. 87-90 MINIMAL INVASIVE EXCISION OF INTRAORBITAL DERMOID CYST Bekir Atik1, Önder Tan2, Zülküf Kaya3, A Faruk Kıroğlu3 Yüzüncü Yıl University, Faculty of Medicine, Departments of Plastic and Reconstructive Surgery1, and Otorhinolaryngology3, Van, Atatürk University, Medical Faculty, Department of Plastic and Reconstructive Surgery2, Erzurum, Turkey Correspondence: Dr.Bekir Atik. Yüzüncü Yıl Üniversitesi Tıp Fakültesi, Araştırma Hastanesi, Plastik cerrahi Servisi, 65200 Van, Turkey. Phone: 904322167853 E-mail: drbekiratik@yahoo.com Code Number: gm07021 Orbital dermoid cyst is a rare tumor for which the pathogenesis remains unclear. It is usually located in the lateral side of the orbita, and may also rarely be observed in the intraorbital region. In this cases, aggressive treatment is necessary for the success because recurrence rate is high. But it should work delicately because of the risk of the eye damage. We report three cases with intraorbital dermoid cysts who were successfuly treated by using a minimally invasive surgery. Eye movements and visual functions were normal in all patients. No recurrences or complications appeared postoperatively. We think that it is possible to excise dermoid cysts totally using a classical surgical technique, including an anterior approach, by careful dissection under loupe magnification. Key words: Intraorbital, Dermoid Cyst, Non-invasive INTRODUCTION Dermoid cysts are benign tumors that represent the simplest form of teratoma (1). Approximately 7% of dermoid cysts affect the head and neck region, and within this region, they are commonly found along the orbital walls(2). Orbital dermoid cysts occur most commonly along the lateral aspect of the orbit, in approximately 69% of cases. Intraorbital location is relatively rare for these lesions. It is known that the treatment of periorbital dermoid cysts is easier than intraorbital cysts which require more aggressive interventions (3).The choice of surgical approach for the resection of orbital cyst is determined by the cyst position in the orbital space as a rule and the best choice is the most direct approach to orbital tumor. Lateral orbitotomy as the extracranial orbital approach is favorable for radical resection of the tumor, which growth is limited to the anterior, lateral and superolateral orbital segment. (1, 2, 3). We hereby report three cases of intraorbital dermoid cyst, which were totally excised by minimally invasive surgery. CASE 1 A 5-year-old boy was admitted to our clinic with a swelling on the lateral side of the right orbita. This mass was first noticed by his parents during the neonatal period. On clinical examination, a cystic painless mass was detected on the superolateral rim of the right orbit, which did not affect eye movements. Magnetic resonance imaging (MRI) showed a lobulated cystic mass begining from the superolateral rim to the intraorbital area (Figure 1). Based on the clinical and MRI findings, diagnosis was done. The operation was performed under loupe magnification of 2.5 x. The cyst capsule was gently detached from the surrounding tissues by blunt dissection. Then the cyst was completely removed without rupture. Minimal localized edema subsided gradually in the postoperative period. No complication including periorbital hematoma, wound infection and impairment of vision or eye movements was noted postoperatively. Histopathological examination showed abundant adnexa in the collagenous wall of the cyst. A round hair shaft was speckled brown and pink and the lumen contained squamous epithelial debris (squames) (Figure 2). CASE 2 A 3-year-old girl presented with a swelling located under the lateral part of the left eyebrow. On physical examination, painless mass was detected on the superolateral rim of the left orbit. No abnormal visual findings including ptosis, displacement of the globe, restriction of the eye movements, or diplopi was determined. A cystic encapsulated mass unrelated to the globe and bone structures was well demonstrated at the superolateral side of the orbit by coronal and axial slices of computed tomography(CT) (Figure 4) Under general anesthesia and loupe magnification, the mass was reached through a transverse incision of 1 cm between the eyebrow and lateral canthus. It was dissected carefully from the surrounding tissues and totally removed. After hemostasis, primary repair was achieved. No complication was encountered postoperatively. A definitive diagnosis of dermoid cyst was made by histopathological examination. CASE 3 A 5-year-old male presented with a swelling located under the lateral part of the right eyebrow. On physical examination, painless mass was palpated on the superolateral rim of the right orbit. No abnormal visual finding was detected. Magnetic resonance imaging (MRI) showed a lobulated cystic mass located from the superolateral to the intraorbital area (Figure 1). Based on these findings, diagnosis was done. Under general anesthesia and loupe magnification, the mass was reached through a transverse incision of 1 cm between the eyebrow and lateral canthus. The mass was dissected carefully from the surrounding tissues and totally removed. A definitive diagnosis of dermoid cyst was established by histopathological examination. The mean of follow-up time were 10 months (12, 10, 8). No recurrence was noted on physical examination and control MRI in any of the patient (Figure 3). Postoperative esthetic outcomes were satisfied all the parents. Eye movements and visual functions were normal after operations in all patients. DISCUSSION Several types of orbital cystic lesions, which can be detected in the childhood period, have been classified by Shields and Shields in 2004 (4). Dermoid cyst is by far the most common orbital cystic lesion in children, accounting for over 40% of all childhood orbital lesions and for 89% of all orbital cystic lesions in childhood that come for biopsy or surgical removal (3). It can usually be found superotemporally near the zygomaticofrontal suture. It develops along the line of embryonic fusion of the naso-optic groove, enfolding the ectoderm during embryonic development. Intraorbital dermoid cysts are very rare pathologies (5), representing 5–10% of all orbital dermoid cyst cases (6,7). Dermoid cysts along the frontozygomatic suture may extend through the lateral orbital wall to produce a dumbbell-shaped lesion (8). The incidence of dumbbell dermoids is very low; a recent report of 65 consecutive cases of frontozygomatic dermoid cysts described only one case of extension through the bone into the orbit (1). CT for orbital dermoids reveals adjacent bone changes in 85% of cases, and a bony defect may be identified radiographically in dumbbell dermoids (5). On occasion, a deep orbital dermoid cyst can occupy much of the orbit (9). Some deep- orbital dermoid cysts remain clinically occult until adulthood, when they enlarge and produce proptosis or medial displacement of the globe. Occasionally, a dermoid cyst can extend through the roof of the orbit into the frontal sinus. Orbital dermoid cysts frequently leak material from the cyst into the surrounding tissues, producing inflammatory signs and simulating a primary inflammation (4). In some cases, a secondary fistula between the cyst and the skin may allow the contents of the cyst to drain intermittently (10). In our cases we encountered none of the complications mentioned above. It is generally accepted that surgical treatment of dermoid cysts is more difficult than that of other periorbital cysts because of their localization and complications. These may not be excised totally and recurrence may be unavoidable. Carta et al. (11) suggested posterolateral orbitotomy to prevent this complication. However, this invasive approach is known to increase mortality and morbidity. We think that it is possible to excise dermoid cysts totally using a classical surgical technique, including an anterior approach, by careful dissection under loupe magnification. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07021f4.jpg] [gm07021f1.jpg] [gm07021f3.jpg] [gm07021f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}