 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
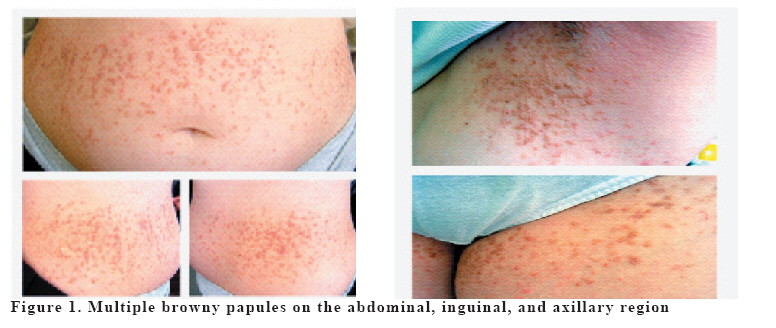
European Journal of General Medicine, Vol. 4, No. 2, 2007, pp. 95-97 IS PRURUTIS TRIGGER BANDLIKE PATTERN DARIER DISEASE: POSITIVE KOEBNER PHENOMENON? Cihangir Aliağaoğlu1, Ali İhsan Güleç2, Ümran Yıldırım3, Hülya Albayrak1 Düzce University, Faculty of Medicine, Department of Dermatology1 and Pathology3, Düzce, Osmaniye State Hospital, Department of Dermatology2, Osmaniye, Turkey Cihangir Aliağaoğlu. Department of Dermatology, Düzce University, Faculty of Medicine, Düzce, Turkey. Phone: 905335695517 E mail: caliagaoglu@yahoo.com Code Number: gm07023 Darier’s disease is an uncommon autosomal dominant genodermatosis characterized by corrupted keratinisation of the epidermis, nails and mucous membranes. A 35-year-old female patient had papular lesions on axillary, inguinal and abdominal regions. The lesions on abdominal region appeared after pruritis. Histopathologic examination of the lesion was consistent with Darier’s disease. Key words: Darier’s disease, Koebner phenomenon INTRODUCTION Darier disease (DD) is an autosomally dominant skin disease characterized by follicular and extra follicular greasy hyperkeratotic papules and plaques that arise primarily in seborrheic areas. Vegetating papules, erosions or hemorrhagic blisters may sometimes be detected. Other findings may include some different nail abnormalities, ‘cobblestoning’ of the oral mucous membrane, punctate keratoses on the palms and soles, and deteriorated papillary lines. Salivary stones, cysts of the long bones, various neuropsychiatric abnormalities and low IQ levels, any one or more of these features, have been reported in some cases (1). Recently, DD pathogenesis linked to mutations in the gene encoding the sarco-endoplasmic reticulum calcium ATPase pump (SERCA2). Defects in calcium signaling within keratinocyte differentiation result in characteristic acantholytic dyskeratosis (2-4). In 1872, Koebner reported a patient in whom, 5 years after developing psoriasis, noted that various traumatic insults to his skin resulted in lesions of psoriasis. The Koobner response is observed in many other skin diseases such as lichen planus and lichen nitidus (5). Up to now, aggravation has been detected in classic predilection region of disease from the cases (heat, humidity, U.V B, trauma) reported in literature (6-8) and did not have a band-like pattern. In our case, the lesions thought to be Koebner-positive were not on classic predilection region and appeared after pruritis. CASE The first lesions in our 35-year-old female patient occurred on the axillary and the inguinal region when he was 18-year old, and the lesions on the periumblical region arose 6-7 months later. The lesions appeared on peri-umbilical region 7 months ago. His family history was negative. On physical examination, multiple small papules were found on the right and left abdominal regions, the axillary and inguinal regions. (Figure 1). The biopsy of a papular lesion showed follicular epidermal invagination, villi, papillary projections, multiple warty dyskeratoma-like structures, suprabasal separation, corps rond, and grains (Figure 2). Nail changes and oral lesions were absent. Findings of the physical examination, including complete neurologic and ophthalmologic examinations, were unremarkable. His complete blood count, urine and stool examinations, and liver and kidney function tests were within normal limits. Serology for VDRL and HIV antibody was non-reactive/negative. Our patient has taken acitretin 1mg/kg for four months ten years ago. He had also been given some long term antibiotic treatments. No obvious healing was ever observed on the lesions. DISCUSSION DD has some clinical variants include hypertrophic, vesicobullous, hypopigmented, cornifying, zosteriform or linear, acute, and comedonal subtypes (9). The typical and distinctive clinical lesion is a firm, rather greasy, crusted papule that is tan-colored or yellow–brown. Coalescence of the papules makes up irregular warty plaques or papillomatous masses, which, in the flexures, become hypertrophic, fissured and malodorous. The predilection sites of DD are the seborrhoeic areas of the trunk and face, scalp margins in particular. Punctate keratoses and minute pits may be seen in palms and soles. Darier’s disease may become worse with age, but severity is unpredictable and its prognosis is changeable. Pruritus is common, occurring in 80% of patients, and may be intractable; however pain is unusual (6). DD becomes worse in the summer frequently, with heat and humudity as the major factors, and can be exacerbated by ultraviolet B (photo-Koebner) light and mechanical trauma, e.g, under the collar of sweater. Most cases tend to improve or clear in winter. Because of the skin erosions, there are frequently severe and excessive itching and discomfort in patients; the factors also cause pain, bleed readily, and have an offensive odor. Lithium carbonate has been reported to induce Darier’s disease in some individual (8). A case triggered by scabies was reported in literature (7). In our patient, the lesions were on axillary, inguinal and peri-umbilical region. Although axillary and inguinal involvements are familiar, the band-like involvement of peri-umblical region is uncommon. We learned from the history of our patient that there had been lesions localized on umbilicus at first and then after severe itching, the new lesions appeared and these made up band-like involvement. The region was covered part of body and our patient had not been exposed to sun-light with any reasons. And also, our patient had not taken any topical or systemic medication. All of the newer lesions appeared after pruritis. We interpreted this event as Koebner-positive. We had not accepted the lesions on peri-umblical region as linear or segmental because of the lesions were not consistent with Blaschko lines. In conclusion, pruritis triggers DD; it not only aggravates DD but also causes new lesions. Therefore, we think that DD may be evaluated as a Koebner-positive disease. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07023f2.jpg] [gm07023f1.jpg] |
| |||||||||

{kind=link}
{kind=link}