 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
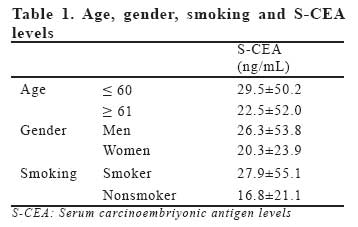
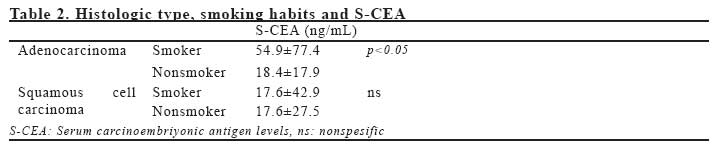
European Journal of General Medicine, Vol. 4, No. 3, 2007, pp. 107-114 SERUM CARCINOEMBRYONIC ANTIGEN LEVEL AS A PREDICTIVE MARKER FOR DISTANT METASTASIS IN NON-SMALL CELL LUNG CANCER Ahmet Ursavaş1, Mehmet Karadağ1, İlker Ercan2, Özlem Özkubat1, Selma Yeşilkaya1, Funda Coşkun1, R.Oktay Gözü1 Uludağ University Medical Faculty, Departments of Pulmonary Diseases1 and Biostatistics2, Bursa, Turkey Code Number: gm07026 Aim: Elevated serum CEA (S-CEA) levels are sometimes attributable to the production of CEA by malignant cells, and in turn, the antigen itself can enhance the metastatic potential of malignant cells. We investigated the predictive role of S-CEA level for distant metastasis in nonsmall cell lung cancer (NSCLC).
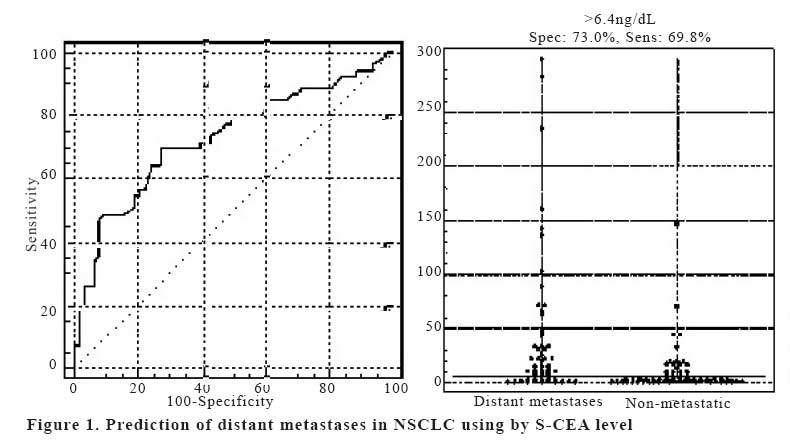
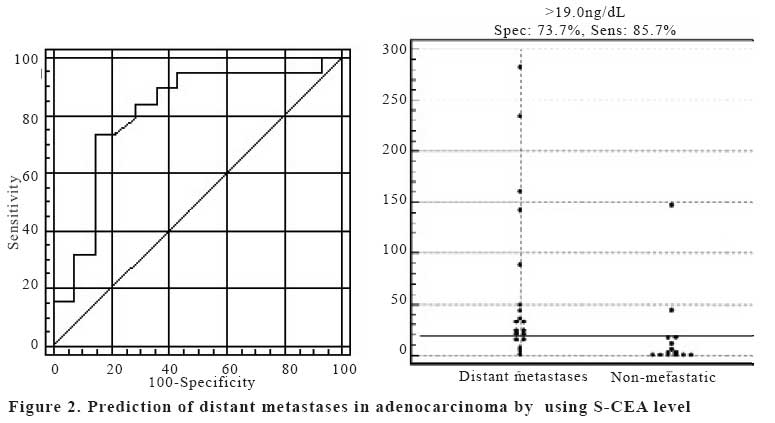
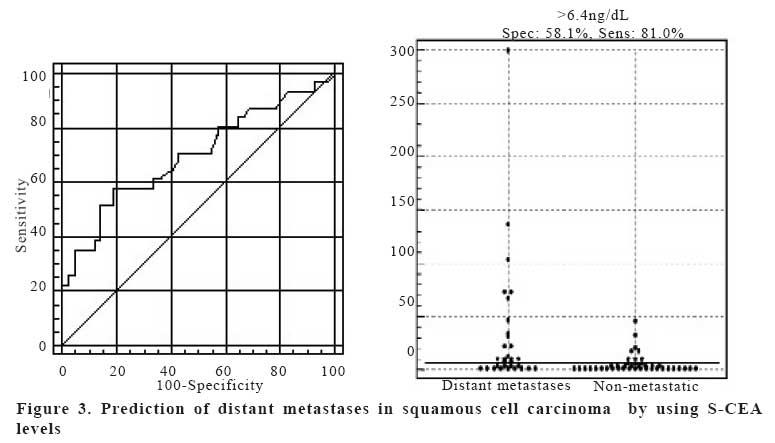
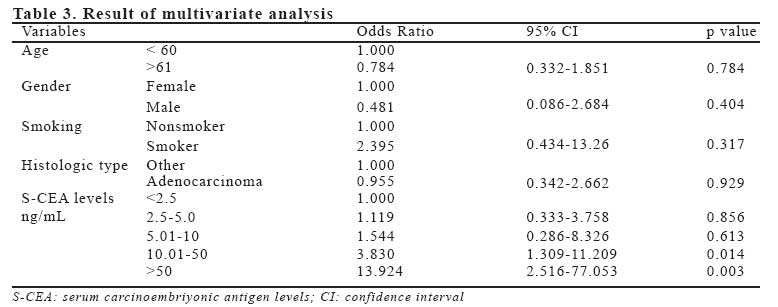
Key words: CEA, lung cancer, distant metastases INTRODUCTION Tumor markers have been used for diagnosis, screening, staging, and monitoring the effects of treatment in cancer. Carcinoembriyonic antigen (CEA) is glicoproteine that defined by Gold and Freedman in 1965 (1,2). CEA has been extensively studied, particularly in regard to its potential role as a marker of early cancer and as a prognostic indicator. The initially interest in CEA was for colon cancer, subsequent studies have shown that S-CEA level may be elevated in many other cancers (3). There is no spesific tumor marker in lung cancer. S-CEA level also do not appear to be sensitive or spesific enough to be useful for screening or diagnosis in lung cancer (4). Furthermore, occasionally S-CEA levels are elevated in patients with nonmalignant diseases such as chronic bronchitis, emphysema, or colitis (5). However, in early stage non-small cell lung cancer (NSCLC), several reports have indicated that elevated preoperative S-CEA levels are associated with more advanced disease and with very poor survival (6-10). Elevated S-CEA levels can occur when the antigen is produced by malignant cell, and in turn, CEA can enhance the metastatic potential of otherwise weakly metastatic cells (11). Tomita et al (12) reported that S-CEA level was not always related to TNM stage but there were significant differences in S-CEA level between M0 and M1 NSCLC patients. Initially staging is a critical step in choosing the optimal therapeutic approach for patients with NSCLC. Many studies have concluded that as many as 30% of who undergo resection for cure have silent distant metastases (13). To perform bone scanning, cranial CT/MR and PET are controversial on pretreatment evaluation in patients who have no symptomps or other evidence of distant metastasis (14). We hypothesized that a cut off CEA level existed that could be used to identify patients with distant metastasis; in addition we speculated this cutoff level would be useful in decision to pretreatment evaluation of distant metastases. MATERIAL AND METHODS Consecutive 116 patients who have histological proven NSCLC referred to our department during the period 2002 to 2005 were investigated retrospectively. Patients with small cell lung cancer or other primary cancers were excluded from this study. Data were collected from patients medical records, with age, gender, smoking history, height, weight, body mass index (BMI: weight (kg)/ height(m)2), symptoms of distant metastases, histologically type and clinical disease staging. All patients included in the study had undergone the routine extrathoracic metastases screening procedures of our clinic. The clinical stage had been determined by using the following: chest computed tomography (CT) including the liver and adrenal glands, fiberoptic bronchoscopy, brain CT scan or magnetic resonance, and whole-body bone scintigraphy. The clinical stage was determined according to the International System for Staging Lung Cancer adopted by American Joint Committee on Cancer and International Union Against Cancer in 1997 (15). The medical records of patients were reviewed to determine clinical factors suggestive of distant metastases. Non-organ specific factors include anemia, leukocytosis, thrombocytosis, hypoalbuminaemia and weight loss (>10%). Organ specific clinical factors were headache, nausea, personality change, seizure, abnormal neurologic examination, bone pain, tenderness, right upper quadrant pain, hepatomegaly, elevated alkaline phosphatase, calcium, transaminase or bilirubin levels. S-CEA levels were measured by using enzyme-linked immunosorbent assay kits. According to the manufacturer, the average for this assay in healthy individuals is 1.93 ng/mL and upper limit of normal is 5.0 ng/mL. S-CEA levels was compared according to age, gender, smoking habits, histological type, distant metastases and clinical disease stage in all patients. S-CEA cutoff levels which predicted distant metastases was determined. Finally we investigated the predictive distant metastases value of S-CEA levels in NSCLC patients who have symptomatic and asymptomatic metastases. Statistical analysis Statistical analysis was performed using the SPSS package for Windows, version 13.0. The evaluation of categorical variables was analyzed by Chi-square test and Fisher-exact test. The statistical significance of differences between the subdivided groups was analyzed by Mann-Whitney U and Kruskal-Wallis test. The relationship among variables was evaluated by Pearson correlation coefficient. Diagnostic propotions were given along with their 95% confidence intervals (CI). To asses the capability to predict distant metastases we used the receiver-operating characteristic (ROC) curves, whose circumscribed areas (the area under the curve) give an estimate of the test’s diagnostic efficiency. A p value less than 0.05 was considered statistically significant. RESULTS One hundred-eighteen patients consisted of 102 men and 14 women with mean age of 60.5±10.2 years (range 39 to 87 years). There were no significant difference between men and women, young (<60 years) and old, and smoker and nonsmokers in terms of S-CEA levels. S-CEA levels of these groups are shown Table 1. There were 33 (28.5%) adenocarcinoma, 73 (62.9%) squamous cell carcinoma and 10 (8.6%) other type NSCLC. S-CEA levels significantly higher in patients with adenocarcinomas than in those with squamous cell carcinoma (45.2±69.6 versus 17.2±41.2 ng/mL; p=0.005). When evaluated S-CEA level, smoking habits and histologic type of tumor together, there were no significant difference between smoker and nonsmokers for both adenocarcinomas and squamous cell carcinomas. Histologic type, smoking habits and S-CEA are summarized Table 2. In patients with NSCLC a significant difference in S-CEA level was observed between stages I-II (6.29±6.45 ng/mL), stage III (10.9±16.2 ng/mL) and stage IV (37.5±64.9 ng/mL) (p<0.05). There were also significant differences in S-CEA level between M0 (10.2±21.3 ng/mL) and M1 (43.8±67.9 ng/mL) (p<0.001). However we could not find significant differences in S-CEA levels between T1-2 and T3-4 (p=0,141), N0-1 and N2-3 (p=0,672). There were fifty-one patients who had distant metastases. The site of distant metastases were, bone in sixteen patients, brain in ten patients, liver in four patients and surrenal gland in four patients. Seventeen patients had multipl metastases. There were no significant difference between site of distant metastases in terms of S-CEA levels. Fortyone of 51 patients who had distant metastases presented at least one organ-specific clinical factor suspicious of metastases. S-CEA levels were not significantly different between symptomatic and silent metastatic NSCLC patients (83.4±132.7 versus 28.4±34.1 ng/mL; p=0.103). We used ROC analysis for the determination of S-CEA levels that can predict distant metastases. In NSCLC, the area under the ROC curve was 0.728 (p<0.001) for S-CEA (Figure 1 A, B). S-CEA threshold of 6.4 ng/mL predictive sensitivity and specificity for distant metastases as, respectively, 69.8% (95% CI: 55.7% to 81.7) and 73.0% (95% CI: 60.3% to 83.4%). In squamous cell carcinoma, the area under the ROC curve was 0.699 (p<0.01) for S-CEA (Figure 2 A, B). S-CEA threshold of 6.4 ng/ mL predictive sensitivity and specificity for distant metastases as, respectively, 58.1% (95% CI: 39.1% to 75.4) and 81.0% (95% CI: 65.9% to 91.4%). In adenocarcinoma, the area under the ROC curve was 0.810 (p<0.001) for S-CEA (Figure 3 A, B). S-CEA threshold of 19 ng/mL predictive sensitivity and specificity for distant metastases as, respectively, 73.7% (95% CI: 48.8% to 90.8) and 85.7% (95% CI: 57.2% to 97.8%). The result of multivariate analysis including age, gender, smoking status, histologic type and S-CEA level are summarized in Table 3. Of the variables that were included in the multivariate analysis, only S-CEA levels qualified as an independent predictive factor for distant metastases. DISCUSSION Serum tumor markers may be helpful in the diagnosis, pathologic classifications, and evaluation of the stage of disease and prognosis. In lung cancer, tumor markers fall into several categories including oncofetal proteins, structural proteins, enzymes, cell membrane components, secreted peptides, hormones and other tumor associated antigens (16). But there is no specific tumor marker that sufficient to reliably detect occult disease or influence the treatment in lung cancer. For this reason, The American Thoracic Society and The European Respiratory Society jointly published guidelines did not recommend routine measurement of any biomarkers in the screening, staging and evaluation of disease progression in lung cancer (17). The role of CEA in lung cancer was first postulated in 1970s (8). Some investigators have reported that elevated preoperative S-CEA levels are predictive of recurrence and indicative of poor prognosis for patients with surgically resected NSCLC (18-21). But other studies involving similar patients cohorts have found that elevated preoperative S-CEA levels are only marginally predictive or completely lacking in prognostic value (22-24). S-CEA levels may be elevated due to nonmalignant disease such as chronic bronchitis, emphysema, or colitis (5). The factor most strongly influencing the increase of S-CEA levels was reported to be cigarette smoking. Alexander et al (25) found correlation between smoking and S-CEA levels, with levels being significantly higher in smokers than nonsmokers and with significantly higher percentage CEA levels; furthermore within 3 months of cessation of smoking, S-CEA levels did not appear to be influenced by previous smoking habits, with levels returning to was characteristic of nonsmokers. Okada et al (26) reported that among nonsmokers, the rate of CEA positive patients was 21.5% for adenocarcinoma and 20% for squamous cell carcinoma. In contrast among smokers the rate of CEA positive patients was 49.3% for adenocarcinoma and 43.8% for squamous cell carcinoma. They suggested that in more than half of CEA positive smokers, S-CEA was increased by cigarette smoking. In our study there was no significant difference between smoker and nonsmokers in termes of S-CEA levels. The relationship between S-CEA levels and tumor histologic type remains controversial. Several reports have indicated that S-CEA levels are significantly higher in patients with adenocarcinoma as compared to patients with squamous cell carcinoma (26-29). Okada et al. (26) reported that although S-CEA levels were significantly higher in patients with adenocarcinoma than in those with squamous cell carcinoma, but the proportion of CEApositive patients with adenocarcinoma (35.3%) was less than that of CEA-positive patients with squamous cell carcinoma (41.9%). They speculated that the majority of CEA-positive patients with squamous cell carcinoma had marginally positive levels of CEA, and consequently that the specificity of the CEA test was low for squamous cell carcinoma patients. In our study, we found significantly higher S-CEA levels in adenocarcinoma than squamous cell carcinoma, in agreement with previous report. In addition, when S-CEA level, smoking habits and histologic type of tumor evaluated together, there was no significant difference between smoker and nonsmokers of adenocarcinoma or smoker and nonsmokers squamous cell carcinoma. Elevated S-CEA levels can occur when the antigen is produced by malignant cell, and in turn, CEA can enhance the metastatic potential of otherwise weakly metastatic cells (11). The reported results of correlation between S-CEA levels and TNM staging in NCSLC are obscure despite extensive studies (6-12). Some authors suggested that S-CEA levels may be correlated with tumor size, vascular invasion of tumor, hiler or mediastinal lymph node and distant metastases in NSCLC. Salgia et al (27) reported S-CEA levels were significantly lower in patients with early stage disease as compared to patients with unresectabl or metastatic disease. Tacamochi et al (30) identified clinical and radiologic predictors of N2 disease, they found that SCEA levels and maximum tumor dimension were more significant in predicting N2 disease than lymph node size on CT scan. They recommended to perform mediastinoscopy in patients with S-CEA level>5 ng/mL and maximum tumor dimension>20 mm. Nonaka et al (31) reported S-CEA level reflected tumor size, but not tumor invasion. Though S-CEA level did not reflect hilar lymph node metastases, patients with mediastinal lymph node metastases had higher S-CEA levels. Recent studies have indicated that elevated S-CEA are associated with more advanced disease and with poor survival (12, 31-35). Okada et al (34) measured S-CEA levels before and after surgery in 1000 consecutive patients with clinical stage I NSCLC who underwent resection of tumor. They found that the survival rate was significantly poorer for patients with a high preoperative S-CEA level and failure to normalize S-CEA levels after surgery. In this study there were 13 patients who preoperative S-CEA level greater than 50 ng/mL among 1000 patients diagnosed as having clinical stage I disease. Of them, 9 (%69) had distant metastases as initial recurrence, and had already died of cancer. Sawabata et al (35) evaluated 242 patients who were diagnosed with pathologic stage IA NSCLC. In their study Subnormal postoperative S-CEA levels were found to be an independent prognostic factor. They suggested that the prognostic value of S-CEA levels may be attributable to enhancement of the metastatic potential of malignant cells by S-CEA, or alternatively, the elevation in S-CEA may be indicative of the presence of malignant cells. Some studies have reported that S-CEA levels were significantly higher in patients with metastatic (M1) disease as compared to patients with nonmetastatic (M2) disease (12, 16, 27). In our study we could not find significant differences in S-CEA levels between T1-2 and T3-4, N0-1 and N2-3. There was significantly higher S-CEA levels in M0 patients when compared to M1 patients. In the present study, we investigated the critical level of S-CEA of predictive significance for distant metastases in NSCLC. Stokes et al (36) reported that patients with a S-CEA levels levels above 40.9 ng/mL (their normal upper limit was 20.9 ng/mL) had recurrence and metastases. Buccheri et al (37) found that preoperative serum assay of CEA was comparable with the pathologic stage of disease and pathologically classified in stage Ia to IIb, a preoperative S-CEA level higher than 10 ng/mL was associated with 67% probablity of tumor relaps. In our study, we determined that S-CEA threshold of 6.4 ng/mL provided a predictive sensitivity and specificity for distant metastases as 70.9% and 73.0% respectively. We conclude that S-CEA levels were significant for predicting distant metastases especially when higher than 6.4 ng/mL. The Joint Statement of American Thoracic Society and the European Respiratory Society on pretreatment evaluation of NSCLC advocates no preoperative imaging of the distant metastases in patients who have no symptoms or other evidence of distant metastases (17). But recent studies have recommended that routine investigation of distant metastases in all patients with lung cancer (38-40). According to our opinion, high levels of S-CEA (especially higher than 6.4 ng/mL) may be an indication to perform routine investigation of distant metastases even in the absence of symptoms and signs. This allows, with very little cost, the identification of a significant proportion of patients who are at high risk of distant metastases when initially staging. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07026f2.jpg] [gm07026f1.jpg] [gm07026t1.jpg] [gm07026f3.jpg] [gm07026t2.jpg] [gm07026t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}