 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
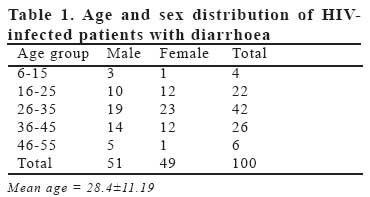
European Journal of General Medicine, Vol. 4, No. 3, 2007, pp. 119-122 CRYPTOSPORIDIOSIS IN HIV INFECTED PATIENTS WITH DIARRHOEA IN OSUN STATE SOUTHWESTERN NIGERIA Yemisi Olukemi Adesiji, Rofiat Omolabake Lawal, Samuel Sunday Taiwo, Sunday Adetona Fayemiwo, Oluwaseyi Adegboyega Adeyeba Ladoke Akintola University of Technology, College of Health Sciences, Department of Medical Microbiology and Parasitology, Osogbo, Nigeria Code Number: gm07028 Aim: Although cryptosporidiosis is said to be rare among adult HIV patients in certain parts of Nigeria, there are no documented studies on the occurrence of this parasite among HIV patients in Southwestern Nigeria.
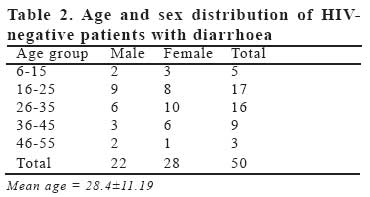
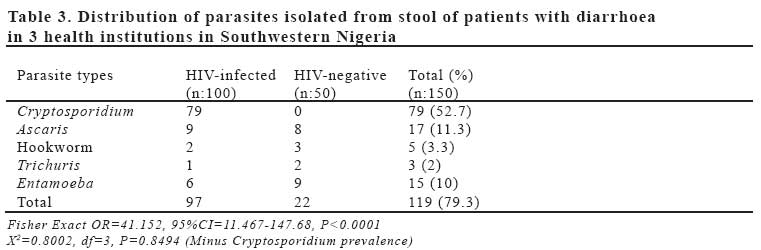
Key words:Cryptosporidiosis, prevalence, Southwestern Nigeria INTRODUCTION Cryptosporidium, an intracellular protozoan has changed from that of a rare largely asymptomatic disease, to an important cause of diarrhoea in animals and humans worldwide (1). Reported Cryptosporidiosis prevalence is 3-4% in the USA (2), 3.5-22.44% in Brazil (3) and about 50% in Africa and Haiti (4). In HIV infected patients, cryptosporidium is the most frequent microbial cause of diarrhea, usually causing chronic bulky and intermittent diarrhoea with liquid non-bloody stools, accompanied by pain and abdominal colic, and a noticeable loss of weight (5) Reports of cryptosporidiosis in Nigeria are few. In North-central Nigeria, Nwabuisi(6) reported prevalence rate of 15.1% among children aged 0-14 years with diarrhoea while Bamwat et al (7) reported a prevalence rate of 4.8% among malnourished children 0-5years. The role of Cryptosporidium in diarrhoea among HIV infected patients in Nigeria has not been established. In one tertiary institution in Southeastern Nigeria (8), no cryptosporidium oocyst was detected in diarrhoea stools of 189 HIV infected and uninfected patients. In Southwestern Nigeria, there are no documented studies on the prevalence of Cryptosporidium among the people. Our study is therefore aimed at determining the prevalence and contribution of Cryptosporidium to diarrhoea among HIV infected patients, the knowledge of which will help in management of HIV related opportunistic infections in our environment. MATERIALS AND METHODS Study area This cross sectional study was conducted in three selected health care facilities in Osun State of Nigeria; State Hospital, Ilesha; Ladoke Akintola University Teaching Hospital, Osogbo and Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife between July and October 2005. Subjects One hundred HIV-infected individuals presenting with diarrhoea were recruited among the patients admitted to HIV or Haematology clinics of the health institutions and 50 HIV-negative individuals with diarrhoea admitted to the medical outpatient or admitted on the wards were included as controls. HIV was diagnosed using a combination of an HIV-1 ELISA screening and a Western blot confirmatory technique or where the latter is not available, using 2 different ELISA methods. Diarrhoea was defined as passage of more than 3 loose or watery stools in 24 hours and was acute if it lasts for less than 14 days and persistent/ chronic if it lasts for 14 or more days(9). Specimen collection Stool samples were collected from each subject into a clean Universal bottle and transported to the medical microbiology laboratory of Ladoke Akintola University Teaching Hospital for analysis. Each subject was interviewed to collect relevant demographic data. Methodology A direct sample of the stool was made with both saline and iodine mounts on clean grease free slides and examined under the microscope first with 10x and then 40x objective lens for ova and cysts of parasites. A sample of the stool was concentrated using formol ether method concentration technique (10). Detection of Cryptosporidium oocysts in the concentrated stool was done using the modified cold Ziehl Neelsen staining technique (11). Briefly, a concentrated smear of the stool was made on a clean grease-free slide and fixed in methanol for 3 minutes. The slide was immersed in cold Carbol fuchsin and stained for 15 minutes. It was then thoroughly rinsed in tap water and decolorized in 1% HCl (v/v) in methanol for 10-15 minutes. After rinsing again in tap water, the slide was counterstained with 0.4% malachite green for 30 seconds. The slide was then air-dried and observed under the compound light microscope using 40x objective lens for the presence of Cryptosporidium oocysts, which was confirmed under the oil-immersion objectives, as small pink to red spherules on pale green background Data analysis Demographic and other data obtained were analysed with a PC containing GraphPad software (GraphPad Software Inc, San Diego, USA). Significant differences between categorical variables were determined using Chi square or Fisher exact tests and P < 0.05 was taken as significant value. RESULTS A total of 150 patients with diarrhoea were investigated for cryptosporidiosis in three health institutions in Osun State, Southwestern Nigeria; 100 (51 males, 49 females, age range 9-54 years, mean age 32.04±9.62) were HIV infected and 50 (22 males, 28 females, age range 9-56 years, mean age 28.4±11.9) were HIV negative and served as controls (Tables 1 and 2). The overall parasite prevalence rate in the diarrhoea patients is 79.3% (119/150) with Cryptosporidium parvum 52.7%, Ascaris lumbricoides 11.3%, Hookworm 3.3%, Trichuris trichura 2% and Entamoeba histolytica 10% (Table 3). The parasite prevalence rate in HIV infected patients is 97% while in HIV-negative patients, the rate is 44%. The rate is significantly higher among HIV-infected patients with diarrhoea than among HIV-negative patients with diarrhoea (OR=41.152, 95%CI=11.467147.68, P<0.0001). However this difference is attributed to Cryptosporidium which was found exclusively among HIV-infected patients. When Cryptosporidium prevalence was excluded from analysis, the parasite prevalence rates between the two groups was not significantly different (X2=0.8002, df=3, P=0.8494). DISCUSSION Diarrhoea is a common complication of HIV infections, inducing weight loss and cachexia and occurring in almost 90% of AIDS patients in developing countries (12). Cryptosporidium is a well established cause of diarrhoea among HIV infected patients worldwide with prevalence of infection ranging from 3% in developed countries to 50% in developing countries (13). However, the role of this parasite in the occurrence of diarrhoea among adult patients with HIV infection in Nigeria is not established. In a study carried out in a tertiary institution in Southeastern Nigeria (8) using modified cold Ziehl Neelsen staining technique, Cryptosporidium was not detected in stool samples of 189 HIV infected and non-infected patients with diarrhoea. This sharply contrasts the finding in our study using the same detection method where an overall Cryptosporidium prevalence of 52.7% is reported and 79% prevalence rate among HIV infected patients. The reason for this large difference can be related to the known fact that HIV opportunistic infections, cryptosporidiosis inclusive, tend to vary from one locality to another and from one country to the other depending on the level of contamination of water, foodstuff and contacts with animals, which are important factors in dissemination of the parasite (14). Cryptosporidiosis in Nigeria has been reported from tertiary institutions mainly among children in North-central (6, 7, 15) and South-south Nigeria (16). Our study on Cryptosporidium among diarrhoea patients appears to be the first from Southwestern Nigeria involving two tertiary and one secondary health institutions. The Cryptosporidium prevalence rate of 52.7% reported among these diarrhoea patients is similar to rates reported from other African countries(4) indicating that cryptosporidiosis is an important opportunistic parasitic disease causing diarrhoea among HIV infected patients in Nigeria. This is especially so as this parasite was detected in stool samples of only HIV infected patients and this further highlights the association between immunodepression and cryptosporidiosis. Although the overall parasite prevalence rate was higher among HIV infected patients when compared to HIV negative patients with diarrhoea in this study, this was mainly due to the high Cryptosporidium prevalence of 79% among the HIV infected patients. When this was removed, the prevalence rates of other parasites were not significantly different among the HIV infected and HIV negative patients. The mechanism by which Cryptosporidium cause diarrhoea is not well known. Inflammatory response to the infection is variable and may be modified by co-pathogens such as Cytomegalovirus. However, histologic evidence of gastrointestinal mucosa injury has been reported with clinical manifestations influenced in part by the anatomic distribution of the infection with extensive infections involving both small and large intestines producing the most severe illness (17) Contrary to a previous report of apparent rarity of Cryptosporidium infections in certain part of Nigeria (8), our study revealed a high prevalence of this parasitosis among HIV infected patients in Southwestern Nigeria. ACKNOWLEGDEMENT We are grateful to Mr. Amure-the Chief technologist of Ladoke Akintola University Teaching Hospital who assisted in processing the specimens and the entire staff of the Department of Medical Microbiology of the Hospital. Also, the staff and management of Osun State Hospital, Ilesha and Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Nigeria who facilitated collection of stool samples from the patients. The study is significant because in Southwestern Nigeria, there are no documented studies on the prevalence of Cryptosporidium among the populace. Our study is therefore aimed at determining the prevalence and contribution of Cryptosporidium to diarrhoea among HIV infected patients, the knowledge of which will help in management of HIV related opportunistic infections in our environment. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07028t2.jpg] [gm07028t3.jpg] [gm07028t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}