 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
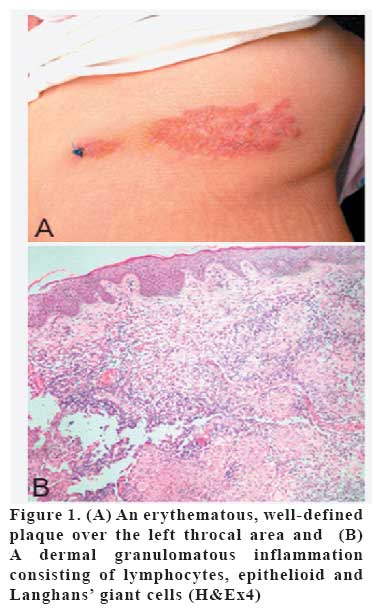
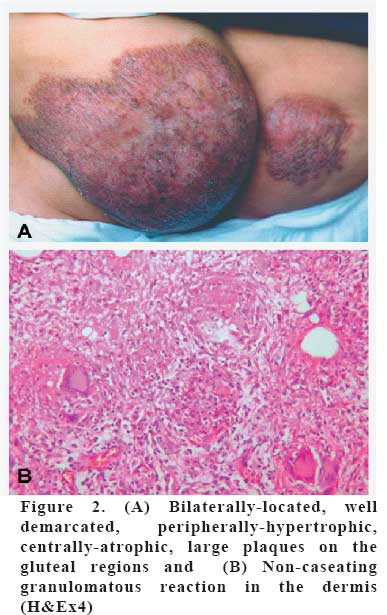
European Journal of General Medicine, Vol. 4, No. 3, 2007, pp. 135-137 LUPUS VULGARIS WITH UNUSUAL INVOLVEMENT Cihangir Aliağaoğlu1, Mustafa Atasoy2, Ümran Yıldırım3, R. İsmail Engin2, Handan Timur2 Düzce University, Faculty of Medicine, Departments of Dermatology and Pathology3, Düzce,Atatürk University, Faculty of Medicine, Department of Dermatology2, Erzurum, Turkey Code Number: gm07031 Lupus vulgaris is the most encountered form of cutaneous tuberculosis, and the most common site of involvement is the head and neck. In our lupus vulgaris cases, the lesions were located in throcal area in one case and gluteal area in the other. Ziehl-Neelsen and periodic acid-Schiff stains did not demonstrate any acid-fast bacilli. Culture did not grow mycobacterium tuberculosis except in case 1. PPD was strongly positive in all of the cases. Lesions of lupus vulgaris improved after anti-tuberculotic threrapy. Key words: Lupus vulgaris, unusual involvement INTRODUCTION Lupus vulgaris (LV) is usually the result of dissemination from an endogenous focus during a period of lowered resistance and mycobacterium tuberculous bacillemia in a previously sensitized host with a strongly positive delayed hypersensitivity to tuberculin (1). LV is often located on the face. Other sites of predilection are the nose, ears, chin, neck, and, rarely, extremities, buttock and trunk. It is more common in females than in males, with all age groups equally affected (2). In our LV cases, the lesions were located in throcal area in one case and gluteal area in the other. There were no active organ tuberculosis and other skin tuberculosis in our cases. CASE 1 A 60-year-old woman was admitted to our clinic with the complaint of long-standing erythmatous lesion over the left of the thoracal area of 20-year duration. Preceding trauma or associated constitutional features, abdominal pain, anorexia or weight loss were not present. Her personal and family histories were not contributory. No diagnosis had been established and no treatment had been given throughout 20 years long. Dermatological examination revealed an erythematous, nontender, well-defined plaque, 20x30 cm in size, present over the left of the thoracal area (Figure 1A). Diascopic examination gave an apple-jelly appearance. The systemic examination was normal. Lymph nodes were not palpable. No BCG scar was visible. The entire dermis was composed of non-caseous granulomatous inflammation which contains epitheloid histiocytes, lymphocytes, and large numbers of Langhans type giant cells (Figure 1B). A Mantoux test was positive with erythema and induration of 18 mm after 48 hours. Mycobacterium tuberculosis was cultured from the biopsy specimen. CASE 2 A 40-year-old woman was admitted to our clinic with the complaint of long-standing, slowly enlarging, painless, and atrophic plaque on the right and left buttocks. The first lesion had appeared approximately 15 years earlier on the right buttock. The lesion was gradually spreading the left buttock. No diagnosis had been established and no treatment had been given throughout this long period. Her personal and family histories were not contributory. Dermatologic examination of the skin surface revealed bilaterally-located, diffuse, well demarcated, peripherally-hypertrophic, centrally-atrophic, large plaques on a violaceous base on the gluteal regions (Figure 2A). Diascopic examination gave an apple-jelly appearance. No BCG scar was visible. Systemic physical examination was normal. Lymph nodes were not palpable. An incisional biopsy specimen of the plaques showed a dermal granulomatous inflammation consisting of lymphocytes and epithelioid cells. However, no caseation necrosis was present (Figure 2B). A Mantoux test was positive with erythema and induration of 20 mm after 48 hours. In all cases, sputum, stool and urine cultures were negative. Laboratory tests showed a normal blood count. VDRL and HIV tests were negative. Fungal and standard bacterial cultures from the skin biopsy were negative. Ziehl-Neelsen and periodic acid-Schiff stains did not demonstrate any acidfast bacilli. Chest radiography and abdominal ultrasound did not show any pathologic finding. Underlying bone and joint disease was excluded by scintigraphy. In addition to these findings, the chest radiography showed right apical calcifications which were considered to be residues of past pulmonary tuberculosis in case 2. The patients were treated with four drugs therapy consisting of pyrazinamide (25mg/ kg), isoniazid (5mg/kg), rifampin (10mg/ kg) and ethambutol (15mg/kg) daily for two months, followed by dual therapy with isoniasid and rifampin for six months. Their cutaneous lesions significantly regressed by leaving hypertrophic and atrophic scars after treatment respectively. DISCUSSION LV is characterized by macule or papule, with a brownish-red colour and soft consistency that form larger plaques by peripheral enlargement and coalescence. If untreated, LV course may continue many years and lead to significant impairment of function and disfiguration. Common areas of LV are the face, ears and neck and may heal with scarring (3). In Europe over 80% of lesions are on the head and neck, particularly on the nose and cheek (4). In Turkey, for example, localization of LV lesions on the face is 62% (5). Cutaneous tuberculosis was scarcely seen on extremities, buttock, and trunk (6,7). The spread is mostly hematogenous or lymphatic. The contagious spread is also seen particularly in cervical adenitis or pulmonary tuberculosis, or sometimes in exogenous infection at the site of primary inoculation or after BCG vaccination (1). Sehgal et al (8) suggested that LV is probably occurred by direct inoculation of the tubercle bacilli into the abraded skin in a sensitized host, and suggested a diagnosis of secondary inoculation cutaneous tuberculosis for this entity. In our LV cases, the lesions were located in thoracal area in one case and gluteal area in the other. The case of throcal LV do not has any tuberculosis focus. We think that the lesion had developed with direct inoculation. There were calcification areas which were thought as old tuberculosis on chest X-ray of the case 2. We think that the lesion had developed from this focus via bacillemia. The differential diagnosis of LV includes sarcoidosis, deep fungal infections, lympcytoma cutis, tertiary syphilis, leprosy, lupoid leishmaniasis, discoid lupus erythematosus, and lichen simplex chronicus (2,3,6,7,9). In the upper dermis of skin lesions, tuberculoid structures, composed of epitheloid cells, Langhans giant cells and mononuclear cells are present histologically. Cutaneous necrosis is slight; tubercle bacilli are sparse and rarely found. The culture can be negative in a significant number of cases of LV. The Mantoux test is positive in most cases of LV. When the Mantoux test is negative, however, it should be regarded as a sign of possible visceral involvement (4). The diagnosis of cutaneous tuberculosis in our current cases suggested by clinical, histological findings, good response to treatment were obtained although microbiological investigations, including acid-fast bacilli staining and culture of case 2 was negative. An 82-year old man with a 71-year history of a large plaque of LV on his chin and upper neck was described in a report. An untreated hypertrophic LV on the upper arm of 67 years’ duration has been described. In an other report, a 65-year old Mexican man with disseminated tuberculosis, who was discovered to have a slowly enlarging annular LV on his buttocks and thighs which escaped diagnosis for 28 years was described. An unusual fungating, ulcerated form of LV on the forehead of a 42-year-old South African man which had been present for 12 years was also reported. An ulcerated form of LV on the buttock of a 87-year-old Caucasian women which had been present for 87 years was an other case (9). In Turkey, a 60-year old man with an atrophic form of LV on the buttock which had been present for 25 years was reported (6). The duration of lesions was long lasting in our patients. In conclusion, tuberculosis is still an important health problem in underdeveloped and developing countries due to the poor hygiene conditions, low socio-economic level and late application of patients for health care which also increases morbidity. REFERENCES
Copyright 2007 - Medical Investigations Society The following images related to this document are available:Photo images[gm07031f2.jpg] [gm07031f1.jpg] |
| |||||||||

{kind=link}
{kind=link}