 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 145-148 Evaluation Of The Diagnostic Criteria Of Restless Leg Syndrome In Hemodialysis Patients Şeref Yüksel1, Mehmet Çölbay1, Mehmet Yaman2, İhsan Uslan1, Gürsel Acartürk1, Özcan Karaman1 Afyon Kocatepe University, School of Medicine, Departments of Internal Medicine1 and Neurology2, Afyon, Turkey Code Number: gm07035 Aim: In diagnosis of restless leg syndrome (RLS), seen frequently in hemodialysis patients, minimal criteria of International RLS Study Group have been commonly used. Our purpose is to investigate the significance of minimal criteria of International RLS Study Group for the diagnosis of RLS in hemodialysis patients in our district.
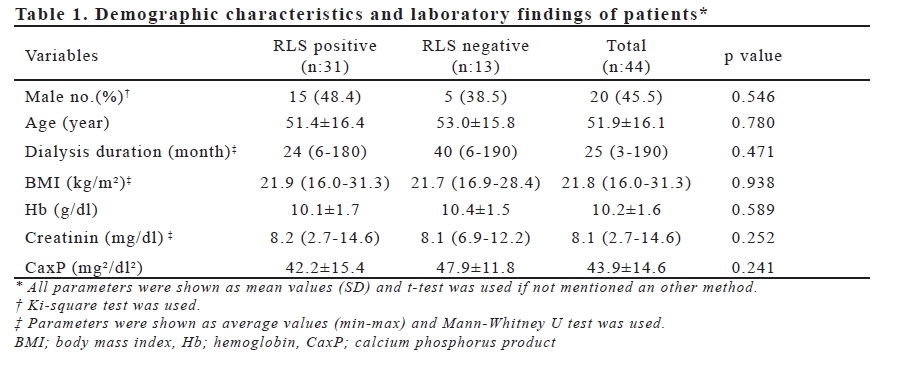
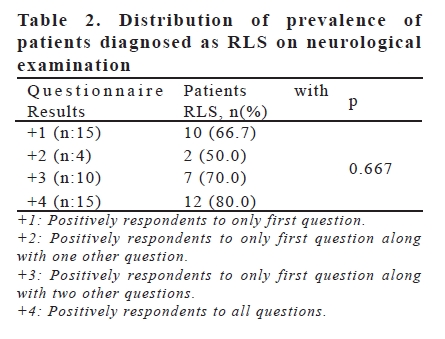
Key words: Restless leg syndrome, hemodialysis INTRODUCTION Cardiovascular complications are one of the most common causes of anesthesia-related morbidity (1). The hemodynamic consequences of drugs and the techniques used for induction of anesthesia have been well documented (2-6). Laryngoscopy and endotracheal intubation are often mandatory for patients undergoing a variety of surgical procedures. It is well known that laryngoscopy and endotracheal intubation following induction of anesthesia is almost always associated with hemodynamic changes due to sympatho-adrenal stimulation (7,8). This increased sympatho-adrenal activity normally causes hypertension, tachycardia or myocardial ischemia in patients with coronary artery disease, intracranial tumors and previous myocardial infarction (9). This increase in blood pressure and heart rate are usually transitory, variable and unpredictable. Transitory hypertension and tachycardia are generally of no consequence in healthy individuals, but either or both may be hazardous to those with hypertension, myocardial insufficiency or cerebrovascular diseases (10). Many pharmacological methods have been devised to reduce the extent of hemodynamic events including high dose of opioids such as fentanyl, remifentanil, alfentanil (11-13), alpha- and beta-adrenergic blockers (14,15), and vasodilatation drugs like nitroglycerine (16). Each of these drugs has a unique advantage and disadvantage in blunting the pressor response to intubation. During the last decade, calcium and sodium channel blockers has been utilized to mitigate the hemodynamic responses to intubation. Diltiazem is one of the calcium channel blockers being used as antianginal, antiarrythmic and antihypertensive agent. Lidocaine (lignocaine) is a common local anesthetic and a sodium channel blocker known to reduce pressor response to intubation. Although these two drugs have been used in various studies alone or combined with other opioids, only two reports have so far examined the benefits of combining both calcium and sodium channel blockers. The first study looked at the combination of these two drugs only in hypertensive patients (10). Based on an English-translated abstract, a second study by Lee et al. (17) also appeared to look at the combination of these two drugs. However in their work, the researchers only measured the heart rate and mean arterial pressure which sharply contrasted with what we found in our study. The present work was undertaken to compare the effect of diltiazem, lidocaine and combination of these two drugs on blunting the hemodynamic responses to endotracheal intubation in normotenseive patients. Because the mechanism for control of hemodynamic changes is different between these two drugs (18,19), we hypothesized that significantly less circulatory responses would be experienced by patients receiving both than receiving either lidocaine or diltiazem alone. MATERIAL AND METHODS This study was undertaken at K.R.Hospital attached to Government Medical College, Mysore, coming under Rajiv Gandhi University of Health sciences, Bangalore, Karnataka state, India. Following institutional approval by the ethical committee at Mysore Medical College, informed consent was obtained from 120 patients. The study population consisted of randomly selected ASA physical status I or II male and female adults, between the ages of 18-60 yr, which were scheduled for various elective surgical procedures. Patients having pre-existing systemic disorders, ischemic heart disease, hypertensive heart disease, diabetes mellitus, bronchial asthma, previous myocardial infarction, renal disease, cerebrovascular insufficiency or association with any co-morbid disease were excluded from the study. Study design Each patient was randomly assigned to one of four study groups. Group I received a single 0.2 mg/kg IV bolus of diltiazem diluted to 5 mL with normal saline 1 minute prior to laryngoscopy and intubation (n:30). Group II received a single 1.5 mg/kg IV bolus of lidocaine (lignocaine) diluted to 5mL with normal saline 3 minutes prior to laryngoscopy and intubation (n:30). Group III received a combined single IV bolus containing both 0.2 mg/kg of diltiazem and 1.5 mg/kg lidocaine diluted to 5mL with normal saline 1 minute prior to laryngoscopy and intubation (n:30). Group IV served as control and received a single 5ml IV bolus dose of normal saline given 1 minute before laryngoscopy and intubation (n=30). Heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial pressure (MAP) were recorded via a Siemens SC-7000 multi-channel monitor for each patient prior to administration of the study drug, at pre-induction and after intubation at the time increments of 1, 3 and a maximum of 5 minutes as after surgery has commenced, multiple factors like various surgical stimuli may also play role in hemodynamic response. Rate Pressure Product (RPP) was calculated and evaluated as well. The rate pressure product was calculated by multiplying heart rate with systolic blood pressure. Restless legs syndrome (RLS) is a extremities, often associated with discomfort disorder of lower extremities characterized and restlessness, 2-occurrence or worsening by marked discomfort and refers to symptoms of symptoms at rest, 3-relief of symptoms of spontaneous, continuous leg movements completely or partly during activity, 4associated with unpleasant paresthesias. occurrence or worsening of symptoms only The symptoms occur only at rest and cause in the evening or at night (10). However in sleep disorder (1). RLS is common among end-stage renal failure peripheral neuropathy dialysis patients with a reported incidence of related to uremia is frequently seen (12). 6.6 to 58.3 percent (2-8). In dialysis patients Consequently neurological examination is with restless leg syndrome quality of life is also important in hemodialysis patients for decreased and risk of mortality is increased, diagnosis of RLS. In fact Crignotta et al this adds to importance of the disorder (9). reported in their studies that in patients with Restless leg syndrome is a clinical chronic dialysis, sensitivity and specificity diagnosis rests on subjective symptoms of diagnostic criteria of International Study in the presence of a normal neurological group was low (7). However this is the only examination. The International Restless study in this patient group. Our purpose in Legs Study Group proposed the following this study is to investigate the significance of four features as minimal criteria for the minimal criteria of International RLS Study Group for the diagnosis of RLS in hemodi alysis patients in our district. MATERIALS AND METHODS We have conducted our study in three dialysis units in city center of Afyonkarahisar. In these dialysis units 68 hemodialysis patients have fulfilled informed consent forms. Socio-demographic characteristics and laboratory values of patients were provided from hospital registries and measurements in last month were used. We investigated each of the criteria of International RLS Study Group for the diagnosis of RLS in each participant. Twenty four patients replied the first question negatively, RLS was not considered in these patients, so other three questions were not asked and questionnaire was finished. Forty four hemodialysis patients replied the first question positively, questionnaire for minimal criteria for the diagnosis of RLS including 4 questions was completed and neurological examination was planned. All patients were examined by the same neurologist. A questionnaire with additional 12 questions including clinical specifications of leg complaints and questioning relations between these complaints and sleep was applied. Subsequently, patients those have RLS according to questionnaire of 4 questions and gold standard neurological examination was studied. SPSS 10.0 packet program was used for statistical analysis. All parameters were summarized by descriptive statistics. In comparison of continuous parameters in groups with or without restless leg syndrome T-test or Mann-Whitney U tests were used and for categorical comparison Chi-square test was used. To compare prevalence of RLS in the same study group according to questionnaire and neurological examination McNemar test was used. P values <0.05 were considered as statistically significant. RESULTS Among 44 (20 men, 24 women) hemodialysis patients mean age was 51±16.1 years and median dialysis period was 25 months (range 3-190 months). Sociodemographic characteristics and laboratory findings of patients were shown in Table 1. In neurological examination of these patients answered positively to first question of questionnaire including minimal criteria for diagnosis of restless leg syndrome 31 (%70.5) patients were accepted as RLS. Between patients with or without restless leg syndrome according to neurological examination, there were no significant differences for age, dialysis period and other characteristics (Table 1). According to answers on questionnaire, patients were classified as positively respondent to first question along with one other question, positively respondent to first question along with two other questions and positively respondent to all questions. Distributions of patients diagnosed as RLS on neurological examination in each group were shown in Table 2. There were no significant differences between RLS prevalence in groups (p=0.667). According to minimal criteria for diagnosis of RLS number of patients considered as positively responded to all four questions was 15 (34.1%); however number of real patients determined on neurological examination was 31 (70.5%). In the same group difference between RLS prevalence determined according to these two criteria was statistically significant (p = 0.001). DISCUSSION RLS is frequently seen in chronic renal failure and hemodialysis patients. In diagnosis of RLS, easy and practical minimal criteria of International RLS Study Group were used. In studies with hemodialysis patients, prevalence of RLS was reported between 6,6% and 58,3% according to these criteria (2-8). In our study including 68 hemodialysis patients 22% of patients were diagnosed as RLS. Even though minimal criteria of International RLS Study Group is frequently used for diagnosis of RLS in hemodialysis patients, Crignotta et al have shown that these criteria were not reliable for diagnosis of RLS in hemodialysis patients (7). In this study, in patients positively responded all four questions sensitivity and specificity of these criteria were %44.7 and %81.6 respectively. Sensitivity and specificity of these criteria were also low in patients positively responded to one, two or three questions. There is no other study investigating significance of minimal criteria of International RLS Study Group for diagnosis of RLS in hemodialysis patients. When the distribution of patients diagnosed according to minimal criteria of International RLS Study Group and neurological examination was concerned, it was seen that the proportion of patients diagnosed as RLS on neurological examination was 2 times higher than the proportion of patients diagnosed as RLS on questionnaire (70,4% and 34,1% respectively). The reasons for the lower proportion of RLS diagnosis based on minimal criteria may be mild complaints and complaints not considered seriously by patients. Consequently, real RLS patients might erroneously assessed on questionnaire and RLS diagnosis might be failed. RLS was diagnosed according to the neurological examination in 66% of patients answered positively only to first question, in 50% of patients answered positively to 2 questions, in %70 of patients answered positively to 3 questions and %80 of patients answered positively to all four questions. This result showed that minimal criteria of International RLS Study Group might give false negative and false positive results in HD patients for diagnosis of RLS. Twenty percent of patients those answered positively to all four questions on questionnaire have not been diagnosed as RLS on neurological examination; the reason for this might be any other leg complaints such as paresthesias, pain, itching, cramps and peripheral neuropathy in these patients. This might lead to false positive RLS diagnosis. In our study we confirmed that RLS has more frequently seen in HD patient group. In these patient groups, minimal criteria of International RLS Study Group frequently used for RLS diagnosis were shown to cause false negative and false positive results as in study of Crignotta et al. Based on questionnaire, in 31.4% of 44 patients RLS was diagnosed however on neurological examination %70.5 of these patients RLS was diagnosed. Therefore, we concluded that patients positively responded at least first question of minimal criteria of International RLS Study Group should also be assessed for RLS in detail. The limitation of the present study was that we excluded the patients answered negatively to first question which was the basic one of the questionnaire. Studies including neurological examination of all patients by a neurologist should provide stronger information in this subject. In conclusion, a true diagnosis is very important for RLS as it affects quality of life, morbidity and mortality in HD patients through sleep disorders. Therefore as well as patients positively responded all four questions, all patients answered positively to at least first question also should be assessed for RLS in detail including gold standart neurological examination. REFERENCES
Copyright 2007 - European Journal of General Medicine The following images related to this document are available:Photo images[gm07035t1.jpg] [gm07035t2.jpg] |
| |||||||||

{kind=link}
{kind=link}