 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 154-160 Methodologic Validity Of Patient’s History In Establishing The Diagnosis Of Epileptic Attacks Abdülkadir Koçer1, Emel Koçer2, Sultan Çağrıcı3, Eren Gözke4 Düzce University, Faculty of Medicine, Departments of Neurology1 and Psychiatry2, Düzce,
Afyon Dinar State Hospital, Neurology Department3, Afyon, Istanbul Fatih Sultan Mehmet
Teaching Hospital, Neurology Department4, İstanbul, Turkey Code Number: gm07037 Aim: We tried to determine the specificity and sensitivity of history in the diagnosis of epileptic seizures in outpatient clinics specialised on epilepsy.
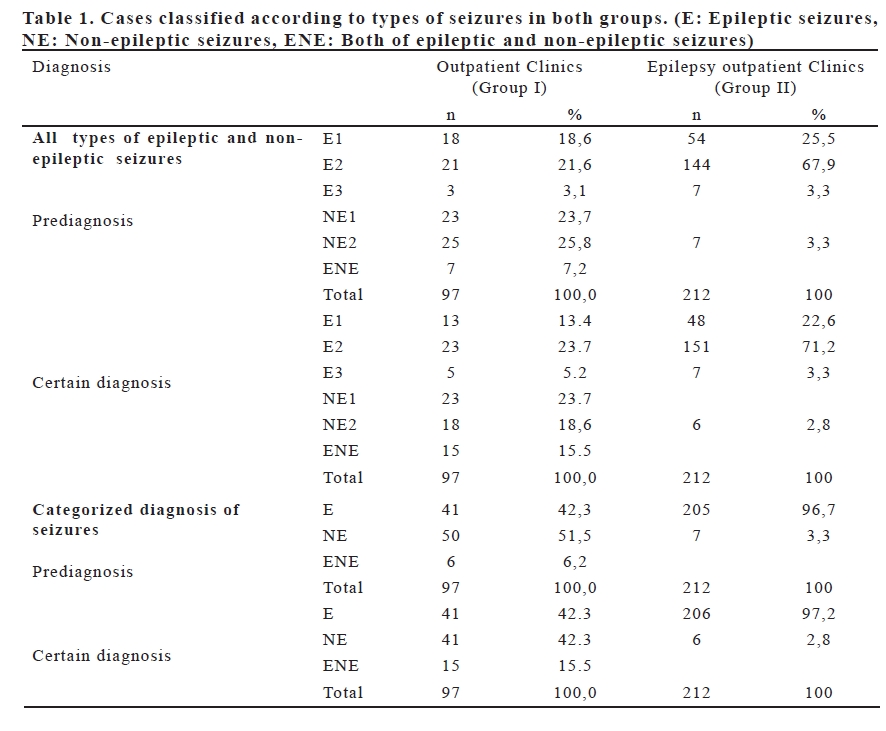
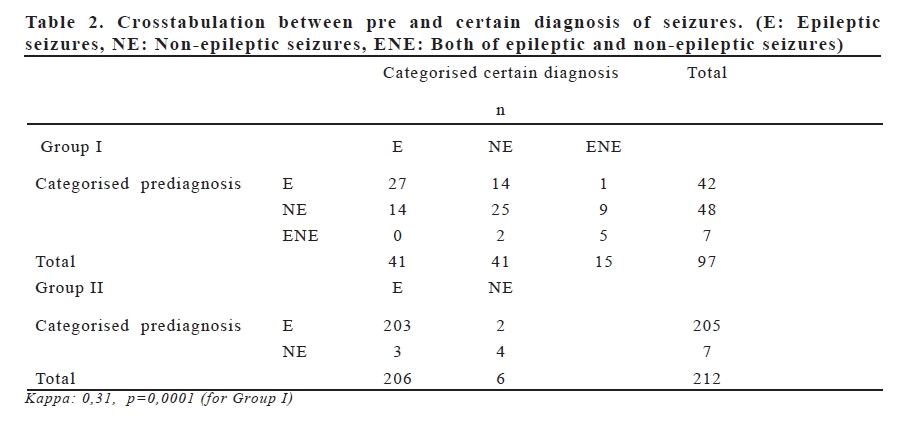
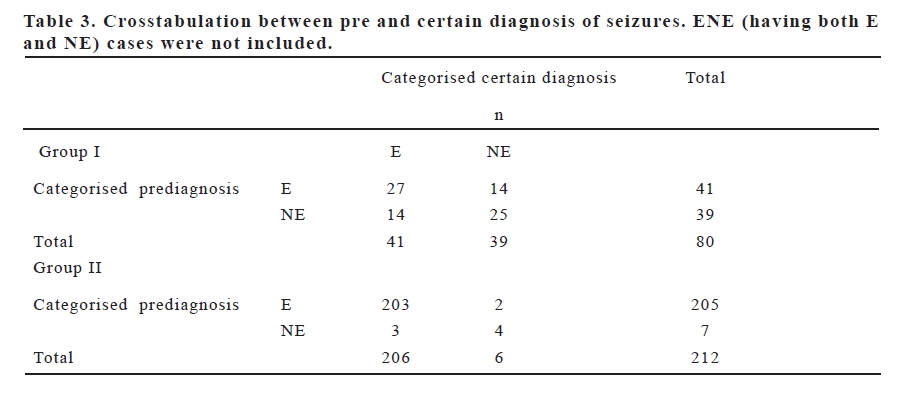
Key words: Conversion disorder, epilepsy, psychophysiologic disorders, seizures INTRODUCTION Epilepsy is a chronic brain disorder manifesting itself with excessive discharge and recurrent episodes. There are systemic, neurological or psychiatric episodes independent of epileptic neuronal discharges that can be confused with epileptic attacks. Non-epileptic seizures that can be mistaken for epileptic attacks pose an important issue (1,2). Diagnosis of epileptic attacks bases mainly on patient’s history (3). Attacks manifesting themselves only with a few simple EEG findings without any definite characterization are not sufficient for establishing diagnosis. Initiation of treatment without establishing a definite diagnosis is more deleterious than waiting for the clear-cut diagnosis. The importance of determination of limitations of electroencephalography must be kept in mind (3,4). Nowack reported that the cost of follow-up of non-epileptic cases owing to misdiagnoses is 4 billion dollars annually (5). History, physician examination and EEG are required for establishing diagnosis. Accurate history taking depends on physician’s recognition of clinical picture of epileptic attacks. In this study methodologic validity of patient’s history which has an important place in establishing the diagnosis of epileptic attacks in normal outpatient clinics and outpatient clinics specialized on epilepsy were evaluated. The results of two different clinical evaluations were compared by statistical analysis. MATERIAL AND METHODS The patients referred to our epilepsy outpatient clinics who were evaluated in our outpatient clinics and whose initial diagnoses established with physical examination and patients’ history were registered in patient follow-up forms and included in the study. Ninety seven patients (40 males, 57 females) with a mean age of 27.89±17.19 years (Range: 2-78 years) referring to PTT Training and Research Hospital with complaints of fit or fainting were evaluated pro-and retrospectively. As second group, we evaluated 215 patients (125 males, 87 women) with a mean age of 24.97±15.50 (Range: 4-79 years) referring to Dr Lütfi Kirdar Kartal Training and Research Hospital outpatient clinics specialized on Epilepsy with complaints of fit or fainting. Two-hundred and fifteen patients with having diagnosis in epilepsy outpatient clinics were included in Group II. For all of the patients, case histories, clinical findings and initial diagnoses determined by case histories, EEG findings, anti-epileptic medications, last / follow-up diagnoses and results of imaging studies (if available) were recorded. The characteristics of attacks were interrogated with questions addressed at patients and witnesses. Cases with definitive diagnoses established with eye-witnessing of the attacks by physicians in the hospital or with video-EEG monitorization were included in evaluations. Differential diagnoses for epileptic attack and non-epileptic attack were based on former studies and previously accepted data. Fifty two patients in Group I and Sixty seven patients in Group II were diagnosed and their treatments were organized during their hospitalizations. During bouts the patient was stimulated (pinching the nose, opening patient’s eyes passively, pressing finger tips or elevating and dropping his/her hand).Reactive responses were recorded (6). During clinical observation, a sentence or a word was uttered and subsequent remembrance of these phrases by the patient was recorded . Eleven patients in Group I and seven patients in Group II were followed up with video-EEG monitorization and then their diagnoses were established in different epilepsy unit. They then were followed-up by our outpatient clinics. EEG complexes containing spikes and sharp waves lasting less than a few seconds were accepted as manifestations of interictal epileptiform abnormalities. Epileptiform activities observed in association with attacks or during prolonged EEG monitorizations were accepted as ictal EEG abnormalities. In 22 cases saline test was administered for differential diagnosis. The patient was informed that attacks could be stimulated after intravenous saline injection but could be terminated sofort by appropriate interventions. When a new episode emerged, it was terminated with a new saline injection. In this case saline test were considered to be positive(7). During 15 minutes following the onset of an attack prolactin levels of 35 cases were tested. Psychiatric diagnosis was based on DSM-IV diagnostic criteria. Thirty five cases were evaluated by means of psychiatric consultations. Psychogenic attacks and other disorders (e.g. transient ischemic attacks, syncope, symptomatic myoclonus) were classified under the name of non-epileptic attacks. Diagnoses were classified into 3 groups as epileptic seizures (E), non-epileptic seizures (NE) and epileptic seizures associated with non-epileptic attacks (ENE). Initial diagnoses were compared with definitive diagnoses established subsequent to examinations. In order to facilitate statistical analysis and classification, the epileptic seizure group were separated into three parts as named E1 (epileptic attacks, complex partial seizures), E2 (epileptic attacks, generalized tonic clonic), and E3 (other epileptic attacks). If loss of consciousness occurred even once during attacks arising from frontal lobe, temporal lobe and occipital lobe then they were evaluated under the heading of complex partial seizures. During performance of statistical analysis cases experiencing ≤ 5 attacks (absence attacks, epileptic syndromes that can manifest more than one type of attacks and partial attacks) were classified as miscellaneous types. Non-epileptic seizures were evaluated in 2 groups as psychogenic (NE2) and non-psychogenic types (NE1). In consideration of detailed examinations performed (gold standard) for the differential diagnosis of epilepsy methodological validity (i.e. sensitivity and specificity) of meticulous history taking was assessed. RESULTS The results of initial and final diagnoses, following review of the cases and completion of the follow-up protocols, of 97 patients in Group I were summarized in Table 1. Additionally, categorized summary has been shown in Table 2. Following definitive diagnosis, the most frequently observed seizures were generalized tonic-clonic convulsions (n:34, 59.6%) between epileptic attacks including E2 with generalised component and non-epileptic seizures. The most frequently observed periods were psychogenic attacks (n:33, 58.9%) among NE in Group I. Following examinations, in 2 out of 6 cases with observed myoclonic spikes, juvenile myoclonic epileptic syndrome while in remaining 4 cases symptomatic myoclonus due to posthypoxic encephalopathy (n=2), Ramsay-Hunt syndrome associated with myoclonus and ataxia (n:1) and propriospinal myoclonus were diagnosed. The most commonly seen ictal finding during E was latency (n:35, 63.6%) and the most frequently observed post-ictal finding was amnesia (n: 45, 80.4%) relating to moment of episode. Unresponsiveness is (n:23, 69.7% ) among the most frequently seen ictal findings during psychogenic seizures (n:33). Most of the E (n=34, 38%) lasted less than 5 minutes. Physical damage was more frequent (n:22, 22.7%) during E. E sometimes associated with pseudoepileptic attacks and 15 (15.5%) patients had taken psychiatric diagnoses. Those were conversion, anxiety, depression and psychosis. In cases with established diagnosis of conversion increases in vocal tones, whinings or cryings were seen. In all of the cases with generalized tonic clonic attacks, amnesia (unable to remember moments of attacks, unable to recollect and hear words spoken outside) was detected. For 20 cases diagnostic saline tests were applied. Saline test was found to be positive in only one of 12 cases with epileptic attacks and in 6 out of 8 patients with established diagnoses of psychogenic seizures. Blood prolactine levels were measured in 15 cases. Increases in prolactinemic levels were detected in 3 (75%) out of 4 cases with established diagnoses of epilepsy. Hyperprolactinemia was observed in only one (12.5 %) out of 8 cases with diagnoses of nonepileptic attacks and 2 out of 3 (66.6%) ENE cases. When patients experiencing epileptic attacks and also ENE cases were assessed all together interictal EEG pathology was detected in 29 (51.8%) out of 56 patients with epileptic attacks. Interictal EEG abnormalities were not found in 2 cases with generalized tonic clonic, in 7 patients with complex partial and in one case with atonic attacks. In 5 of these cases during video-EEG monitorisation, ictal EEG pathologies were observed. In only 2 cases with nonepileptic attacks interictal EEG abnormalities were detected. The results of initial and final diagnoses, following review of the cases and completion of the follow-up protocols, of 212 patients in Group II were summarized in Table 1. Additionally, categorized summary has been shown in Table 2. In Group II, the most frequently observed seizures were generalized tonic-clonic convulsions (n:171, 80.7%) between epileptic attacks including E2 with generalised component (n:20) following definitive diagnosis. There was no patient having diagnosis of E and NE together. Only 6 patients (0.5% of all patients) had a diagnosis of psychogenic attacks. The most commonly seen ictal finding during E was latency (n:135, 65.5%) and the most frequently observed post-ictal finding was amnesia (n: 185, 89.8%) relating to moment of episode. Unresponsiveness is (n:3, 50%) among the most frequently seen ictal findings during psychogenic seizures (n:6). Most of the E (n:180, 87.4%) lasted less than 5 minutes. Physical damage was more frequent (n:65, 31.5%) during E. Only 6 (0.5%) patients had taken psychiatric diagnosis of depression and psychosis. In all of the cases with generalized tonic clonic attacks amnesia (unable to remember moments of attacks, unable to recollect and hear words spoken outside) was detected as well. For 2 cases diagnostic saline tests were applied and saline test was found to be positive in 2 patients with established diagnoses of psychogenic seizures. Blood prolactin levels were measured in 20 cases. Increases in prolactinemic levels were detected in 16 (80%) out of 20 cases with established diagnosis of epilepsy. When patients experiencing epileptic attacks, the interictal EEG pathology was detected in 139 (67.5%) out of 206 patients with epileptic attacks. In only 1 case with NE, interictal EEG abnormalities were detected. When the patients were classified as epileptiform cases (E and ENE) and others in Group I (Table 3), the sensitivity and specificity of establishing the diagnosis of epilepsy were 65.8% and 64.1% respectively. In other words, positive predictive value could be established for 65.8% of epileptic and negative predictive value 64.1% in our study. Total percentage of accurate diagnosis was found to be 65%, while positive and negative predictive values were 65.8% and 64.1% respectively. In Group II, the sensitivity and specificity of establishing the diagnosis of epilepsy were 98,5% and 66.6% respectively when the patients were classified as epileptiform cases (E and ENE) and others (Table 3). Total percentage of accurate diagnosis was found to be 97.6%, while positive and negative predictive values were 99.0% and 57.1% respectively. DISCUSSION The most reliable information in order to determine whether the clinical picture described with complaints such as fainting or losing himself/herself relates to an epileptic seizure can be obtained from the patient or the witnesses beside the patient during his/ her fainting episode. Data supporting the diagnosis of epileptic seizures are their sudden onset, associated loss of consciousness of repetitive nature which comply with classical seizure descriptions (2,7). Information obtained after clinical investigation related to epileptic seizures (squinting eyeballs, foams coming from mouth, contractions of head and neck muscles, urinary incontinence, biting one’s tongue and confusion after an attack) are important for the diagnosis (1,2,8). In our study patient’s intimates had observedly described especially GTC attacks relatively well. When compared with other types of attacks stereotypic nature of generalized tonic clonic seizures allowed extraction of diagnostic features from anamnesis. Other types of seizures were considered to be more heterogenic as previously reported (9). Psychogenic and epileptic seizures can be encountered in the same person. E can be seen in 10-25 % of cases with NE. In cases with a previous history of E, NE can be observed at various time intervals (1,2,10,11). In our study, Es observedly accompanied 15.5% of the cases with NEs in Group I. Atypical epileptic attacks, disorders of movement and sleep, neurological pathologies due to systemic diseases can be at times misdiagnosed as psychogenic seizures (11,12). Individuals diagnosed as atypical epilepsy are frequently deprived of the chance of appropriate investigation and treatment. Therefore, steps aiming at achieving accurate diagnosis convey much importance. Especially complex partial seizures originating from frontal and temporal lobe can be confused with psychogenic seizures. In our study it was observed that 5 out of 18 cases with initial diagnoses of complex partial seizure were misdiagnosed. Besides final diagnoses of 3 out of 23 cases which were followed as having psychogenic seizures had been determined to be experiencing complex partial seizures. The results of initial and final diagnoses, following review of the cases and completion of the follow-up protocols, of patients in Group I and II were summarized in Table 1. Additionally, categorized summary has been shown in Table 2. As it was seen, E1 (Complex partial seizures) was misdiagnosed mostly in Group I and II respectively. In our study diagnoses of GTC and epileptic syndromes could be established with accurate and complete medical history. The presence of GTC associated with psychogenic attacks were demonstrated. For the cases with myoclonus, in accordance with literature it was concluded that myoclonus should not be considered within the context of epileptic seizures in present study (13). The two most important clinical manifestation that can be confused with epileptic attacks are syncope and psychogenic seizures. Various clinical findings can be directive about psychogenic seizures. Although psychogenic attacks might resemble any type of epileptic attacks, they can commonly progress with convulsions. Psychogenic attacks are commonly encountered in emergency and intensive care units. Absence of any EEG changes despite loss of consciousness, presence of alpha rhythms and its atypical clinical nature are commonly used diagnostic criteria for psychogenic seizures (14). In a study performed by Saygı et al. psychogenic seizures reportedly emerge at older ages (14). In our study mean ages of patients with psychogenic seizures were found to be similar. Unresponsiveness without any motor finding is the most important clinical picture seen during psychogenic seizures (1,6). The rate of unresponsiveness in a study by Leis et al. was reported to be 76 percent, while this rate was found to be 52 % when considered in association with other psychiatric diagnoses in our study (6). Generalized convulsions, lethargy or flaccid collapse support the diagnosis of psychogenic attacks (15,16). During attacks of patients with established diagnoses of psychogenic seizures (conversion) absence of motor movements and relatively unconstrained behaviour were noteworthy. Nonepileptic attacks were usually confused with complex partial seizures. Provocative tests can be helpful especially for diagnosis of NE (17). In our study in 6 out of 8 cases (75%) diagnosed as NE and underwent saline tests, positive results were detected. Hyperprolactinemia are frequently encountered especially in GTC and CP seizures. However absence of hyperprolactinemia doesn’t have diagnostic value (18,19). In accordance with literature, in our cases with epileptic seizures increases in blood prolactin levels were observed. Despite all of these findings differentiation between E and NE can be relatively difficult (1,10,11,17,20-23). Psychogenic seizures don’t have a distinct characteristics. In a study by Leis et al. 68 percent of cases with pure psychogenic seizures were followed with antiepileptic medications (6). Hoefnagels et al. reported that a detailed medical history obtained using a seizure questionnaire form could facilitate differentiation of clinical pictures of Es (8). Togay-Işıkay et al. using the same questionnaire form, reported that they did not adequately differentiate between Es (21). Similarly, Eroğlu et al. emphasized that diagnosis based on only medical history and EEG examination might be misleading and result in unnecessary usage of antiepileptics (4). As supporting all those reports, we found that it was not so easy to diagnose psychogenic seizures and epileptic seizures in Group I. On the other side, they were easily separated from each other in Group II. We thought that this was because of admission to epilepsy clinics after selection in the outpatient clinics. Generally all patients admitted to epilepsy policlinics had come after very intensive investigation periods. Biases are relatively common in differential diagnosis between E and NE. Definitive diagnostic criteria are based on observance of seizures or ictal EEG and video monitorisation. If one imagines that the second alternative is not practical and not used routinely, then the importance of anamnesis gains prominency. In our study, in actual outpatient conditions 65.8% (sensitivity) of epileptic and 64.1% (selectivity) of nonepileptic cases could be diagnosed with medical history. Under normal policlinic conditions (excluding special epilepsy clinics) the rate of establishing accurate diagnosis based on medical history taken without a regular protocol was found to be 65%. Since in a domestic source surveillance study, a similar methodological study was not utilized, the values relating to sensitivity and selectivity could not be compared. Given that medical history would be largely dependent on individual attitudes, experiences and working conditions of physicians, it was concluded that with application of seizure questionnaire forms more carefully in special outpatient clinics, these rates could be higher. The ninety-nine percentage (sensitivity) of epileptic and 57.1% (selectivity) of nonepileptic cases could be diagnosed with medical history in special epilepsy clinics. This may be seen as a higher percentage, it is true. We think that the patients with epileptic seizures were selected and then they were sent to the specialists in the teaching hospitals. Anyway, the rate of establishing accurate diagnosis based on medical history was found to be higher than normal outpatient clinics under excluding special epilepsy clinics. All these findings supported that given priorities to training institutions, clinical evaluations of diagnoses obtained with anamnesis at appropriate time intervals would clearly increase percentages of accurate diagnoses. REFERENCES
Copyright 2007 - European Journal of General Medicine The following images related to this document are available:Photo images[gm07037t2.jpg] [gm07037t3.jpg] [gm07037t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}