 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 161-164 Baseline Iron Status Of Apparently Healthy Children In Port Harcourt, Nigeria Zaccheaus Awortu Jeremiah1, Emmanuel Kufre Uko2, Fiekumo Igbida Buseri1, Teddy Charles Adias1 Rivers State University of Science &Technology, 1Department of Medical Laboratory Science,University of Calabar, 2Department of Haematology & Blood Transfusion, Port Harcourt,Nigeria Code Number: gm07038 Aim: Iron deficiency is one of the micronutrient disorder affecting mostly children in the developing countries. There is paucity of information on this subject in our locality. Aim: This study was aimed at assessing the baseline iron status of apparently healthy children aged 1-8 years in Port Harcourt, Rivers state, Nigeria.
Key words:Iron deficiency, prevalence, ferritin, transferrin, Port Harcourt, Nigeria. INTRODUCTION Iron is an essential nutritional element and plays critical role in oxidative metabolism, cellular growth, oxygen transport and storage (1). Iron deficiency is defined as a condition in which there are no mobilizable iron stores and in which signs of a compromised supply of iron to tissues, including the erythron, are noted. The more severe stages of iron deficiency are associated with anaemia (2). Iron status can be considered as a continuum from iron deficiency with anaemia, to iron deficiency with no anaemia, to normal iron status with varying amounts of stored iron and finally to iron overload which can cause organ damage when severe. Iron deficiency is the result of long-term iron imbalance. Iron stores in the form of haemosiderin and ferritin are progressively diminished and no longer meet the needs of normal iron turnover (1-3). Iron deficiency has been described as the most common single nutritional disorder in the world (4,5), with a prevalence of 39.0% in non-industrialized countries among the under fives and 48.1% among the 5-14 years group (6-8). In 1992, the World Health resolution WHA 45.33 urged member states to “establish, as part of the health and nutrition monitoring system, a micronutrient monitoring and evaluation system capable of assessing the magnitude and distribution, vitamin A and iron deficiency disorders and monitor the implementation and impact of control programmes”(9). In keeping with this resolution, a nationwide food consumption and nutrition survey was conducted in Nigeria in 2001(10). This survey missed out Rivers state as a participant state thus creating an information gap on this subject. This present study was primarily aimed at assessing the magnitude and distribution of iron deficiency among apparently healthy children aged 18 years in Port Harcourt, Rivers State of Nigeria. This information can serve as a basis for planning policies and interventions, and as a baseline against which to assess their impact. Table 1. Mean values of iron status indicators among the 240 children participants
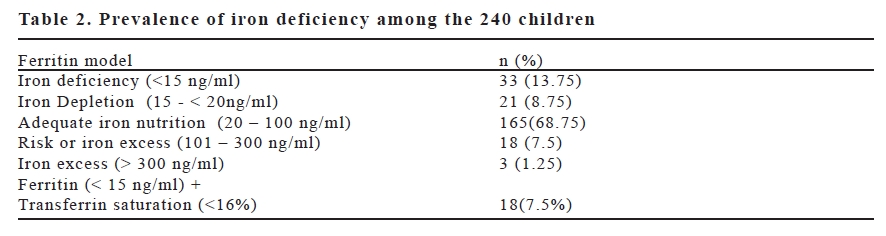
*: p < 0.05, **: p < 0.01, ns : not significance MATERIAL AND METHODS Subjects This study included 240 apparently healthy children aged 1-8 years drawn from the Rumueme community in Port Harcourt, the capital of Rivers State, Nigeria in a prospective cross-sectional survey. The Rivers State University of Science & Technology Ethical Committee approved the study. Informed consents were obtained from parents of selected households. Selection of households was based on random cluster sampling. The parents brought their children to the research base located in Rumueme Port Harcourt where blood samples were collected from them. 117 boys and 123 girls (Ratio 1: 1.05) participated in the study. 3 millilitre of blood was collected by venipuncture into a plain sample container, allowed to clot and then spun to separate the serum. The serum was assayed immediately or frozen at – 80°C in an event of delay in carrying out the analysis. Study Serum iron, total binding capacity and transferrin saturation were estimated by a ferrozine based iron/TIBC reagent set manufactured by POINTE SCIENTIFIC Inc, Canton MI, USA (LOT NO. 516703). The test works on the principle that, transferrin-bound iron is released at an acid PH and reduced from ferric to ferrous ions. These ions react with ferrozine to form a violet coloured complex, which is measured spectrophotometrically at 560nm.The absorbance measured at this wavelength is proportional to serum iron concentration. For, TIBC, a known amount of ferrous ions are added to serum at an alkaline PH. The ferrous ions bind with transferrin at unsaturated iron-binding sites. The additional unbound ferrous ions are measured using the ferrozine reaction. The difference between the amount of ferrous ions added and the unbound ions measured is the unsaturated iron-binding capacity (UIBC). The TIBC is equal to the serum iron concentration plus the UIBC. i.e serum iron concentration + UIBC = TIBC (ugldl). Test procedures were followed as contained in the manufacturer’s standard operating manual inserted in the kit. Transferrin saturation was calculated from serum iron concentration and TIBC values as follows: SI/TIBC x 100 Serum ferritin level The measurement of serum ferritin was done on the archived samples using the human ferritin Enzyme immunoassay test kit. (POINTE SCIENTIFIC INC, USA; LOT NO RN-23128, Expiring 08/2008). The ferritin quantitative test is based on a solid phase enzyme linked immunosorbent assay (ELISA). The assay was carried out on ELISA machine (STAT FAX 2100, AWARENESS TECHNOLOGY INC, USA). Test procedures were followed as contained in the manufacturer’s standard operating manual using point – to – point mode. Results were read from an analog printer Epson LX 300 + (USA) Statistics Results were analyzed with SPSS computer database (Version 10.0 for windows). Mean + standard deviations were used to describe the continuous variables. Student’s t test was used in the comparison of age and sex groups. The statistically significant level was set at alpha 0.05 (p ≤ 0.05). RESULTS Table 1 shows the mean values of the 4 parameters tested. The overall mean values of the variables tested in the study population were serum iron 19.8±21.8 umol/l, TIBC 62.9±46.0 umol/l, transferrin saturation 29.2±18.5% and serum ferritin 50.6±52.3 ug/ml. There was age and sex dependent differences in the mean values of all parameters (p<0.01) except transferrin saturation which did not show any sex dependent statistical difference in the mean values (p>0.05). In table 2, the prevalence of iron deficiency based on the ferritin models is shown. Using ferritin as a single index of iron deficiency, 13.75% were classified iron deficient, 8.75% iron depleted, 68.75% adequate iron, 7.5% risk of iron excess and 1.25% iron excess. Classification of iron deficiency based on the combination of serum ferritin concentration (<15 uglml) and transferrin saturation (<16%) gave an overall iron deficiency of 7.5%. DISCUSSION In normal individuals, the iron used for hemoglobin formation accounts for about two thirds of total body iron. One-third of this body iron may be deposited as haemosiderin or ferritin in stores that can be mobilized when there occurs a need to supply iron in a functionally active form. About 14% of iron is used for other vital physiological functions (11). In addition; a small pool of iron in plasma is in transit and bound to the iron carrier called transferrin (12). Measurement of serum ferritin level has been recommended by WHO (9) as the most specific biochemical test that correlates with relative total body iron stores. A low serum ferritin level reflects depleted iron stores and hence is a precondition for iron deficiency in the absence of infection. The generally accepted cut-off level for serum ferritin, below which iron stores are considered to be deficient is < 15 ugldl (2). In this survey, iron status indicators, serum iron, TIBC, serum ferritin and transferrin saturation were employed in defining the iron status and prevalence among these children. Serum ferritin level and serum ferritin plus transferrin saturation were used to define the prevalence of iron deficiency in this study population. Among children under 5 years of age, the greatest prevalence of iron occurs during the second year of life, due to low iron content in the diet and rapid growth during the first year. This is complicated in developing countries by the presence of parasitic infection like hookworm and malaria (13). In this survey, the mean values of serum iron, TIBC, ferritin and transferin saturation demonstrated age-dependent differences, with values lower in the under fives than the 5 year and above group (p<0.01). Similarly sex related differences in the mean value were observed in all indicators used except transferrin saturation. This supports earlier published reports that children under five years of age are vulnerable to iron deficiency than older children (13,14). The vulnerability to iron deficiency is a function of changes in iron store, level of iron intake and needs relating to growth or iron losses. The earliest age to begin assessment of iron status has been suggested to be between 6 and 9 months (9). The nationwide survey involving 12 states in Nigeria (excluding Rivers State where this study was conducted) in 2001(10) reported that 22.3% of children under five years were iron deficient using single ferritin model as an indicator. Similar prevalence rates of 19.8% and 32.4% have also been reported in Western Kenya and Kazakhstan respectively (15,16). In this study, using a single ferritin model; the prevalence of iron deficiency was found to be 13.5% based on the cut off value of 15ng/ml. With a combination of serum ferritin and transferin saturation, a prevalence rate of 7.5% was obtained. These findings corroborates other reports that iron deficiency among children of under five years of age is a common problem world wide and if left untreated could cause impairment of psychomotor development and alterations in behavior (17-19). REFERENCES
Copyright 2007 - European Journal of General Medicine The following images related to this document are available:Photo images[gm07038t2.jpg] [gm07038t1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}