 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 165-171 Diagnostic Value Of CEA, CA-19-9, CA 125 and CA 15-3 Levels In Malignant Pleural Fluids Gülden Paşaoğlu1, Adil Zamani2, Gülsüm Can3, Oktay İmecik2 State Hospital of Ulus, Department of Chest Disease1, Ankara, Selcuk University, School of Medicine , Departments of Chest Disease2 and Biochemistry3 Konya, Turkey Code Number: gm07039 Aim: Pleural effusion is a common diagnostic problem. Tumor marker levels in pleural effusion may be help to distinguish pleural malignancy, but the precise diagnostic value of these markers remains unclear. The aim of this study was to investigate the diagnostic value of CEA, CA15-3, CA 19-9 and CA-125.
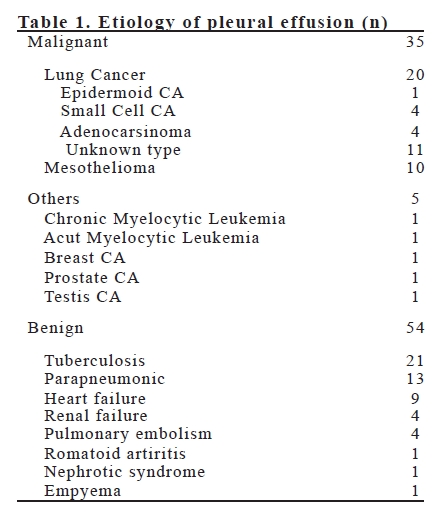
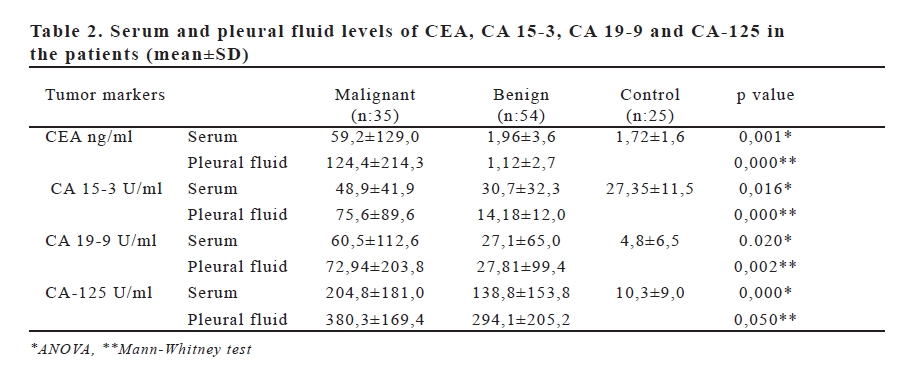
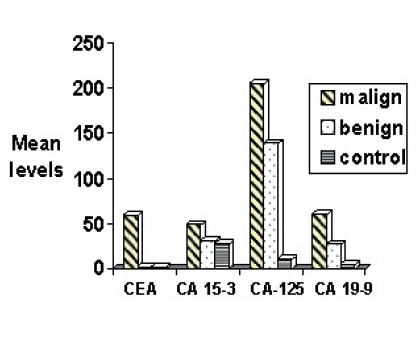
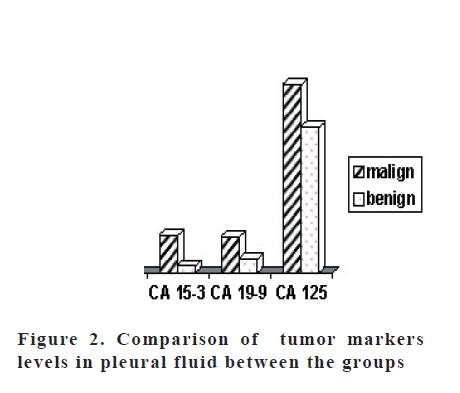
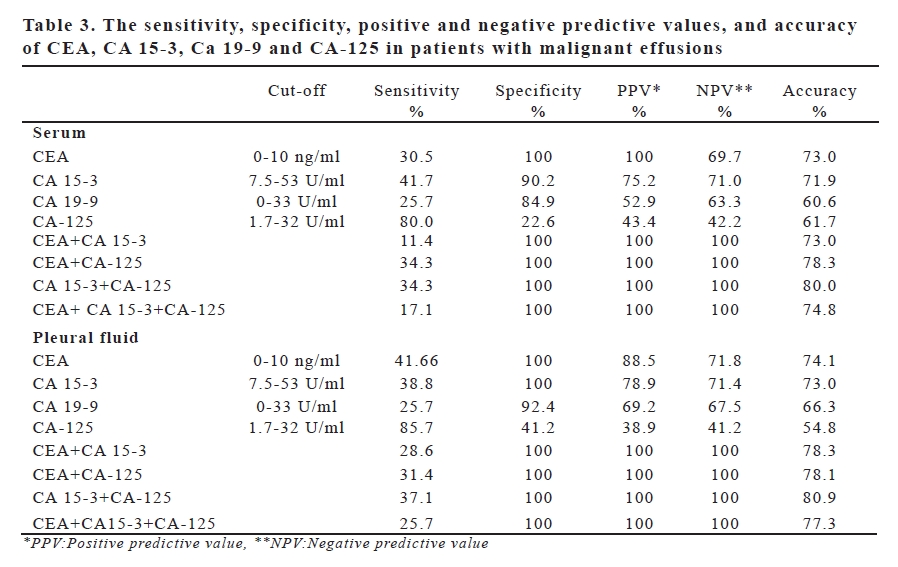
Key words: Tumor marker, CEA, CA 15-3, CA-125, CA 19-9, pleural effusion INTRODUCTION Pleural fluids are encountered as a common complication of many diseases. While 20% of those fluids are malignant, the most common causes are known to be lung (50%) and breast cancers. Non-infectious causes such as heart and kidney failure or infections like tuberculosis and pneumonia, lead to benign pleural fluid formation, as well (1-2). Distinction of those etiological causes as malignant and benign, is considerably important (3). Although it is applied as a standard procedure, cytology examination for diagnostic purposes has a sensitivity of 50-70% (4,5). While thoracoscopy helps to reach a diagnosis with 90% accuracy, it is an invasive, difficult, and costly method (6). Recently, utilization of several tumor markers as a non-invasive method for distinguishing malignant pleural fluids from benign ones, is highlighted. While the frequently recommended and investigated marker to date, CEA, exhibits a specificity around 90%, its sensitivity has been found to be varying between 29-71%. CA 15-3, CA- 125 and CA 19-9 are the other markers that are mentioned to have a diagnostic value. However, different results have been reported for the sensitivity of those markers (7-9). In the present study, it has been aimed to investigate the diagnostic value of CEA, CA 15-3, CA-125 and CA 19-9 on distinction of malignant and benign diseases by measuring their levels in serum and pleural fluids of patients. MATERIALS AND METHODS In a prospective study, 89 consecutive patients with pleural fluid who were admitted to and examined in Chest Diseases Clinic, and 25 healthy individuals, were included. The patients were grouped in 2 as malignant and benign according to their etiological diagnosis. Fluids sampled from patients via thoracentesis who showed presence of pleural fluid in physical and radiologic examinations, were analyzed by biochemical, microbiological, and cytologic methods. Pleural biopsy was performed by Cope needle on cases which are assessed as exudative according to the Light criteria. Moreover, thorax USG, thorax tomography, lymph node biopsy, transthoracal aspiration biopsy, bronchial mucosal biopsy via bronchoscopy, bronchial lavage, sputum cytology, and thoracoscopy were performed for diagnostic purposes when required. Pleural fluid and blood samples were obtained from patients simultaneously; blood samples of the control group were drawn in sitting position between 10.00 -12.00. Serums of blood samples and supernatants of pleural fluids are seperated and stored at -20C in a deep freeze until the date of analysis. CEA, CA 15-3, CA-125 and CA 19-9 levels were determined by “solid phase chemiluminescent immunoradiometric assay” method in Nuclear Medicine Laboratory of Biochemistry Department in Selcuk University. Chemiluminescent enzyme immunoassay kits (Immulite, Diagnostic Products Corporation EURO/DPC-England), have been prepared as specific to each tumor marker antigen seperately. For CEA “Immulite CEA (Cat No:LKCE1)” kits, for CA 15-3 “Immulite BR-MA (Cat No:LKBR1)” kits, for CA-125 “Immulite OM-MA (Cat No: LKOM1)” kits, and for CA 19-9 “Immulite GIMA (Cat No:LKGI1)” kits, were used. By use of standard dilutions, no values above 550 ng/ml for CEA, 300 U/ml for CA 15-3, 500 U/ml for CA-125, and 1000 U/ml for CA 19-9 were observed. Cut-off value for each tumor marker had been determined by the manufacturer of the kit. Cut-off values for CEA, CA15-3, CA, and CA19-9 were 0-10ng/ ml, 7.5-53 U/ml, 1.7-32 U/ml, and 0-33 U/ml, respectively. Statistical analysis were made using the statistical program SPSS 10.0. Data are expressed as means ± SD. Spearman’s correlation coefficients (r) and their corresponding significance values (p) were calculated between the variables. Comparison of the data among three groups was analyzed by ANOVA test and two groups were compared using nonparametric Mann Whitney-U test. Sensitiviy, specificity, positive, and negative predictive values were calculated between patients with and without malignancies. Differences associated with p<0.05 were considered statistically significant. RESULTS While 35 of 89 patients with pleural effusion were determined as malignant, 54 were grouped as benign cases. Mean age was 64.37±10.54 in malignant group, 47.94±15.56 in benign group, and 45.28±11.71 in control group. In malignant group, whereas 24 (65.2%) of 35 patients were male and 11 (34.8%) were female, there was a smoking history in 21 (60%) of those cases. In benign group, while 34 (62.9%) of 54 patients were male and 20 (37%) were female, 28 (48.1%) patients had a history of smoking. Control group was consisted of 13 female and 12 male (48%) individuals; and 11 (44%) individuals had history of smoking. The causes of benign and malignant effusions are shown in Table 1. 20 of 35 patients with malignancy, had primary lung cancer. Whereas 4 of those were small cell lung cancer, 4 were adenocancer, and 1 was epidermoid cancer. Type of lung cancer couldn’t be determined in the remaining 11 patients. Ten patients had mesothelioma and 5 had extrapulmonary cancer. Among 54 patients with benign effusion, the underlying cause was tuberculosis in 21 patients and nonspecific infection in 13 patients. Mean values for CEA, CA15-3, CA-125 and CA 19-9 in serum and pleural fluids of patients with benign and malignant effusions, are shown in Table 2. All the pleural and serum tumor marker levels were statistically significantly higher in malignant group compared to those in benign group (Figure 1 and Figure 2, respectively). A significant correlation was determined between 2 different markers, and between serum and pleural fluid levels of all markers. Highest correlation was found to be between serum and pleural fluid levels of CEA (r= 0.82, p=0.000), however, correlation between pleural fluid and serum levels of CA15-3, CA 19-9 and CA-125 markers was considerable, as well (r=0.69 p=0.000, r=0.61 p=0.000 and r=0.53 p=0.000, respectively). Comparison of tumor marker levels in different cancer types revealed significantly higher CA 15-3 pleural fluid level in primary lung cancer patients compared to those of patients with extrapulmonary cancer (p=0.019). CEA level in primary lung cancer patients was higher, although not statistically significant, than those of cases with extrapulmonary cancer (p=0.059). However, there was no significant difference between primary lung cancer and mesothelioma regarding tumor marker levels (p>0.05). While 50% of primary lung cancer patients had increase of both CEA and CA15-3 levels in pleural fluids, they were high in only 10% of mesothelioma patients. None of the cases with extrapulmonary cancer, had elevated levels of two tumor markers in their pleural fluid. Sensitivity, specificity, negative and positive predictive values and accuracy for each tumor marker can be seen in Table 3. Although sensitivity of CEA was low in both serum and pleural fluids (30.5% and 41.6%, respectively), its specificity (100%, 100%) and accuracy (73.0%, 74.1%) were the highest among other tumor markers. Whereas CA 15- 3 serum and pleural fluid specificity (90.2%, 100%, respectively) and accuracy (71.9%, 73.0%) were similar, CA19-9 serum and pleural fluid specificity (84.9%, 92.4%) and accuracy (60.6%, 66.3%) were a little lower. Specificity and accuracy rates of CA-125 were the lowest values (51.2%, 41.2% and %61.7%, 54.7%, respectively). While the marker with the highest sensitivity (85.7%) was CA125, most specific markers were CEA and CA 15-3 (100% in both) in pleural fluid. When CEA+CA 15-3 evaluated together in pleural fluid, sensitivity was 28.6%, specificity, PPD, NPD were 100% and accuracy was 78.3%. While CEA+CA15-3 + CA-125 combination showed 25.7% sensitivity;100% specificity, positive predictive value (PPV), negative predictive value (NPV); and 77.3% accuracy, CA 15-3+CA 125 combination’s sensitivity was 37.1%; specificity, PPV, NPV was 100%, and accuracy was 80.9%, similarly, CEA+CA 125 combination sensitivity was 61.4%; specificity, PPV, NPV was 100%; and accuracy was 78.1%. DISCUSSION Today, despite all the advances in diagnostic methods, there are still difficulties encountered in differential diagnosis of pleural fluids. Although tumor markers, as a noninvasive method, have been reported to have the potential of being decisive in distinction of malignant fluids in many studies, this is a matter which is still contentious and not clear. In the present study, levels of tumor markers consisted of CEA, CA 15-3, CA 19-9 and CA-125, were significantly high in malignant fluids. CEA was the marker which had the highest specificity (100%) and accuracy (74.1%). CEA+CA 15-3+ CA 125 combination elevated the diagnostic value to 100% specificity and 73% accuracy. The highest diagnostic value was observed in CA 15-3+CA 125 combination (100% specificity and 80.0% accuracy). Moreover, pleural CEA and CA 15-3 levels were significantly higher in patients with primary lung cancer compared to those of patents with extrapulmonary cancer. It is known that synthesis of CEA is increased by malignant cells. It has been suggested that decreased lymphatic drainage due to the obstruction of the lymphatics by malignant cells and pleural invasion may increase the CEA level in pleural fluid (11). A study revealed high CEA levels in 5 patients with negative pleural fluid cytology, and malignant characteristics of those patients were verified eventually by pleural biopsy and VATS. Furthermore, 13 of 21 patients with suspected malignity due to cytology results, showed high CEA levels and all of them were verified to be malignant. Due to those results, use of CEA tumor marker in patients suspected to be malignant, has been suggested (1). Similarly, several studies determined CEA as the tumor marker which has the highest diagnostic value (1,3,12-14). Our results supported this conclusion, as well. CA 15-3, which is more specific for breast cancer, has not been evaluated adequately for malignant pleural effusions. However, several studies showed its specificity to be high (1,3 11,12,15,16). Ghayumi et al. determined CA 15-3 as a marker with high sensitivity and specificity (70% and 83.3%, respectively) along with the highest accuracy (76%) (3). Shitrit et al. found specificity and accuracy of CA 15-3, in their study that including their own patients and patients that they searched of the literature, as high (96.9% and 75.2%, respectively), and cited that it would be one of the specific tumor markers (1). In the present study, pleural level of CA 15-3 was found to be showing high sensitivity (100%) and accuracy (73%) similar to CEA, and our results were observed to be consistent with the international literature. Several investigators highlighted that determination of tumor marker levels might be useful in distinguishing the type of cancer. Wagner et Faravelli, found CA 15-3 level to be higher in patients with metastatic cancer compared to that of mesothelioma cases (17,18). While Porcel et al., found CEA level showing an increase of 59% in lung cancer and 71% in gastrointestinal cancer cases, they determined CA-125 level in patients with ovarium cancer as 67%. Moreover, when evaluated combination of CEA, CA15-3, CA125 and CYRFA 21, they found decisive marker levels in 2/3 of lung and breast cancer patients and in almost all of the GIS cases. In the present study, while CA 15-3 was found to be at a significant level, CEA levels were determined to be higher, although not statistically significant, in patients with primary lung cancer than those of cases with metastatic cancer. However, no difference was detected between tumor marker levels of mesothelioma and primary lung cancer patients. Immunohistochemical studies showed CA 125 is released from pleura and peritoneum. In a few studies CA 125 level compared with other markers, only one of the studies revealed high sensitivity and specificity (19), but others showed high sensitivity, but low specificity for distinguishing malignant fluids; thus, they concluded that CA-125 level was insufficient if used alone for distinction of malignant fluids (1,11,20). In the present study, CA-125 was found to have a high sensitivity and low specificity for malignant fluids. However, when evaluated together with CEA or CA 15-3, whereas its PPV and NPV reached to 100%, its accuracy was found around 80%. Our data supported the previous studies in the literature which indicated its use in combination with other markers such as CEA and CA 15-3 for differentiative diagnosis of malignant fluids. Oligosaccharide (sialo-lacto-Nfucopentaose-II) epitope is related to Lewis a (Lea) blood group antigen. Three percent of overall population is genetically Lea negative and tumor cells of those people can not secrete Ca 19-9. Moreover, increases reaching to 55%, are not sufficient to show that tumor is inoperable. CA 19-9 increases in pleural fluids as a result of an antigenic reaction despite an invasion of serous membranes by a few tumor cells (21). While previous studies found low sensitivity but high specificity for Ca 19-9 level in malignant pleural fluids (1,9,14,15), only Kuralay et al. determined both of them at high levels (19). In the present study, we found low sensitivity and high specificity of CA 19-9 level as well. When all the studies on this subject, including the present one, are evaluated, CA 19-9 was observed to be an inappropriate tumor marker for determining malignancy of fluids. Recently, combinations of tumor markers consisted of 2 or 3 components, are stated to be more sensitive than pleural fluid cytology. Wagner et al., highlighted evaluation of CEA and CA 15-3 combination in serum and pleural fluids, as a more effective method increasing the sensitivity (overall sensitivity 77%) to a value higher than cytopathological examination (69.4%) (16). While Ghayumu et al., obtained highest values (80% sensitivity and 100% specificity) by combination of serum and pleural fluid CA 15-3 levels with pleural fluid NSE and CEA results, Ferrer et al., reported a similar level of sensitivity (65.1%) reached by CEA, CYFRA 21, and CA-125 combination which was more valuable than cytology (56%), and moreover; Villena et al., determined a sensitivity of 64% exhibited by CEA, CA 15-3 and CA 549 combination which was again higher than cytology result (46%) and concluded that such combinations might be helpful in differential diagnosis of malignant fluids (3,9,11). In the present study, similar to others, while CEA and CA 15-3 combination in pleural fluid was determined to display an increase of specificity, PPV, NPV to 100% and accuracy to 78.3%; CEA+CA 15-3 + CA125 combination was found to be manifesting an elevation of specificity, PPV, NPV to 100% and accuracy to 77.3%. The best combination was CA 15-3 and CA 125 which exhibited 100% specificity, 100% PPV, 100% NPV, and 80.9% accuracy. In conclusion, in the present study, pleural fluid marker levels were observed to be significantly higher in malignant diseases, and CEA and CA 15-3 were found to have a high diagnostic value. CA 19-9 and CA-125 had a lower diagnostic value. Furthermore, when markers are evaluated as combinations with each other, their diagnostic value elevated more considerably. CA 15-3 and CA-125 combination had the highest diagnostic value among other combinations. Based on the data we are of the view that that evaluation of tumor marker combinations in order to differentiate malignant pleural fluids from benign ones prior to thoracoscopy additional to cytology, might be helpful to reach an accurate diagnosis and reduce the need for a thoracoscopy. REFERENCES
Copyright 2007 - European Journal of General Medicine The following images related to this document are available:Photo images[gm07039f2.jpg] [gm07039t3.jpg] [gm07039t2.jpg] [gm07039f1.jpg] [gm07039t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}