 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 190-198 Antidiabetic Treatment In Diabetic Patients With Coronary Artery Disease Ahmet Soylu, Mehmet S. Ülgen, Mehmet Akif Düzenli Selcuk University, Meram School of Medicine, Department of Cardiology, Konya, Turkey Code Number: gm07044 The prevalence of diabetes mellitus (DM) that is about 150 million today is estimated to exceed 300 million by the year 2025 (1). When considered that about half of the patients remain undiagnosed, it can be seen how serious the dimensions of the disease are (2). In the patients with DM more than 90% of whom are consisted by non-insulin dependent diabetes mellitus (NIDDM, Type 2 DM), the disease is a significant risk factor for the development of coronary artery disease (CAD) responsible for 75% of all deaths (3,4). In this group of the patients who generally require antidiabetic treatment inevitably, it is highly important to decide on an appropriate treatment due to the various cardiovascular (CV) effects of the anti-diabetics medications and drugs. In order to help establish this decision, in this review it was tried to investigate antidiabetic drugs after a general approach to CAD pathophysology in diabetic patients, especially in terms of their cardiovascular effects. Key words: Antidiabetic treatment, coronary artery disease INTRODUCTION The prevalence of diabetes mellitus (DM) that is about 150 million today is estimated to exceed 300 million by the year 2025 (1). When considered that about half of the patients remain undiagnosed, it can be seen how serious the dimensions of the disease are (2). In patients with DM more than 90% of whom are consisted by non-insulin dependent diabetes mellitus (NIDDM, Type 2 DM), the disease is a significant risk factor for the development of coronary artery disease (CAD) responsible for 75% of all deaths (3,4). In this group of the patients who generally require antidiabetic treatment inevitably, it is highly important to decide on an appropriate treatment due to the various cardiovascular (CV) effects of the anti-diabetic medications and drugs. CAD Pathophysiology in Diabetes Mellitus Insulin resistance and hyperinsulinemia Being an indicator of insulin resistance, hyperinsulinemia is an independent risk factor for the development of CAD (5). Insulin resistance and hyperglycemia can lead to the development of NIDDM, dyslipidemia, hypertension (HT), and atherosclerosis by bringing about the compensatory hyperinsulinemia (6) (Fig. 1). Insulin increases the secretion of endothelial growth factor and endothelin-1, which are strong vasoconstrictor. The effect of insulin normally acting as a vasodilator in the skeletal muscles via secretion of endothelial nitric oxide syntheses is impaired due to insulin resistance (7). Insulin has also been demonstrated to cause proliferation in the smooth muscle cells (8). Hyperglycemia By increasing the production of free oxygen radicals, long-term hyperglycemia: 1) decreases the production of endothelial nitric oxide, 2) causes vasoconstriction and hypertrophy in smooth muscle cells as the result of the increase in production of endothelin and angiotensin II, and 3) activates thrombotic factors (tissue factor, plasminogen activator inhibitor-1 [PAI-1], prostacycline). Besides, the oxidative stress and advanced glycation end-products (AGEs), as the cause of endothelial dysfunction occurring due to hyperglycemia increase the chemotactic factors causing the transmigration into subendothelium of the inflammatory molecules and monocyte (9). Endothelial dysfunction Although the cause of endothelial dysfunction described as an imbalance where vasoconstriction outweighs the vasodilatory properties of the endothelium is not entirely understood, hyperglycemia (10), impaired anti-oxidant balance (11), dyslipidemia and the increase of free fatty acids (12) are thought to cause endothelial damage. Impaired vasodilatation increasing the CV risk exists in the persons with insulin resistance prior to the overt hyperglycemia occurrence (7). The dysfunction of vascular endothelium in charge of vascular tone, vascular permeability and the regulation of angiogenesis plays a major part in many vascular diseases (including atherosclerosis and diabetic microangiopathy as well). Dyslipidemia The level of high density lipoprotein (HDL) decreases while the level of low density lipoprotein (LDL) increases in both insulin resistance and NIDDM. In the presence of hyperglycemia, these LDL particles become glycosylated, and it is difficult to be recognized by the LDL receptors. These LDL particles are scavenged by the tissue macrophages creating the foam cells, a constituent of the atherosclerotic plaque (7). Inflammation Vascular inflammation plays an important role in the development of atherosclerosis and plaque stability (13). Systemic acute phase reactants some of which are found to be related to adverse cardiac results (14) increase in DM (15). Moreover, the amount of “vascular cell adhesion molecule-1 (VCAM1)” independently increasing the coroner risk is also present in diabetics in higher concentrations (16). Prothrombotic state The level of plasma fibrinogen, factor VII, PAI-1 increased in DM, and endogen fibrinolysis decreased (17,18). This situation causes coagulation cascade and platelet activation to strengthen. Besides, thromboses in diabetics are bigger, and more GPIIb/IIla receptors are available on their surfaces. Therefore, they can be aggregated more easily (19). Antidiabetic Drugs Because the hyperglycemia and hyperinsulinemia are well-known risk factors for the CV complications with diabetic patients, taking them under control constitutes the mainstay of the anti-diabetic treatment. The drugs used for this reason are;
Insulin The natural course of NIDDM is the progressive loss of beta cells. Thus, only insulin itself or combination with oral drugs will be needed approximately 10 years after hypoglycemic drug use. Even though there is an obvious relation between endogen hyperinsulinemia and atherogenesis, there is no convincing evidence related to the increased CV disease risk or mortality with the external insulin administration (4). Intensive glucose control treatment (sulfonylurea and/or insulin) decreased microvascular complications 25% in the United Kingdom Prospective Diabetes Study (UKPDS) where intensive glucose control treatment on microvascular and macrovascular complications in patients with newly diagnosed NIDDM was compared with diet treatment (20). However, in macrovascular complications (fatal/non-fatal myocardial infarction and sudden death), 16% (p = 0.052) of risk decrease has been established. No difference is established between sulfonylureas and insulin with respect to cardiovascular events. In the obese group taking metformin, 39 percent of decrease was determined in the myocardial infarction (MI) incidence compared to diet group (21). Moreover, the CV event incidence in those whose HbA1c level is below 7% was found to be lower in this study. In the Diabetes Mellitus, Insulin Glucose Infusion in Acute Myocardial Infarction (DIGAMI) Studies in which standart glycemic control was compared with intensive insulin treatment (four times a day SC insulin for at least 3 months following a 24h insulin-glcose treatment) during and after acute myocardial infarct (AMI) in patients with DM, mortality rate was signicantly less in infusion group (22). This result in favour of the insulin Table 1. Contraindications to metformin therapy (29).
glucose infusion can be explained with some mechanisms (23); 1) this treatment may increase glucose utilisation as an energy source by heart muscle, 2) it decreases the production of free fatty acids which may both spoil ventricular contractions and trigger ventricular arrhythmias by preventing lipolysis, 3) it transforms the cardiac metabolism from free fat acid oxidation into glucolysis. Moreover, a firm glycemic control may reverse the thrombosis activation inducted by hyperglycemia and may decrease PAI-1 activation. Furthermore, some of the positive effects in the insulin-glucose group can be explained with the avoidance from probable harmful cardiovascular effects of sulfonylureas. In the diabetic subgroup analysis of the BARI, the study where the long-term clinical results of coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) were compared in patients with multivessels coronary artery disease, no survival difference was detected between CABG and PCI in those taking only oral antidiabetic drugs, whereas survival rate was found less in the PCI compared to the CABG in those taking insulin treatment (24). Oral antidiabetic drugs Biguanides Metformin as an insulin sensitizer inhibits gluconeogesis, decreases glucose absorbtion from gastrointestinal system (GIS) and increases the peripheral glucose uptake by the tissues (mainly skeletal muscles) in the presence of insuline. Metformin having no direct effect on pancreas β-cells does not cause hypoglycemia. The most common side effect is diarrhea and may increase plasma levels of homocysteine which is a very significant risk factor for CAD by impairing absorption of group B vitamins and especially folate in the chronic treatment (25, 26). Lactic acidosis seen especially in the presence of predisposing factors like Congestive Heart Failure (CHF) is an extremely rare complication of biguanides (27). Metformin can interact with CV drugs commonly used due to its renal excretion. When metformin is used with nifedipin or furosemide, the plasma level of metformin is increased. Digoxin, quinidine and triamterene which are eliminated with renal tubular secretion may also interact with metformin by competing with proximal renal tubular transport systems (28). The contraindications to metformin therapy are summarized in table 1. Metformin as an insulin sensitizer has positive cardiovascular effects (30). It improves the lipid profile (decreases triglyceride [TG] and LDL), fibrinolytic activity, endothelial functions and insulin resistance (31). Contrary to the other antidiabetics, it is preferred for the obese patients as it is not the cause of gaining weight. In the PCI-applied diabetics, a significant risk decrease has been established for any clinical event in those taking metformin at the end of 9 months in a study where the clinical results of the patients taking a sensitizer treatment (whether an additional treatment or not as well as metformin) and taking a nonsensitizer treatment (insulin and/or sulfonylurea) were investigated. In this study where no data about the discrimination of diabetes types could be obtained, the decrease of the risks was more evident at especially the mortality and MI end points (32). Sulfonylureas Sulfonylureas, the hypoglycemic effects of which are directly related to the basal plasma glucose level (33), affect at the cellular level closing the ATP-dependent potassium channels. This feature is responsible for both their insulinotropic effect and their CV side effects. Sulfonylureas are matched with a high affinity to one of the subunits on these channels causing the depolarization of the cells. These channels closed at the physiological conditions cause hyperpolarization which protects the cell from the effects of ischemia opening at the ischemic conditions. Sulfonylureas prevent the hyperpolarization protecting the cell inhibiting the opening of these channels (34). Sulfonylureas;
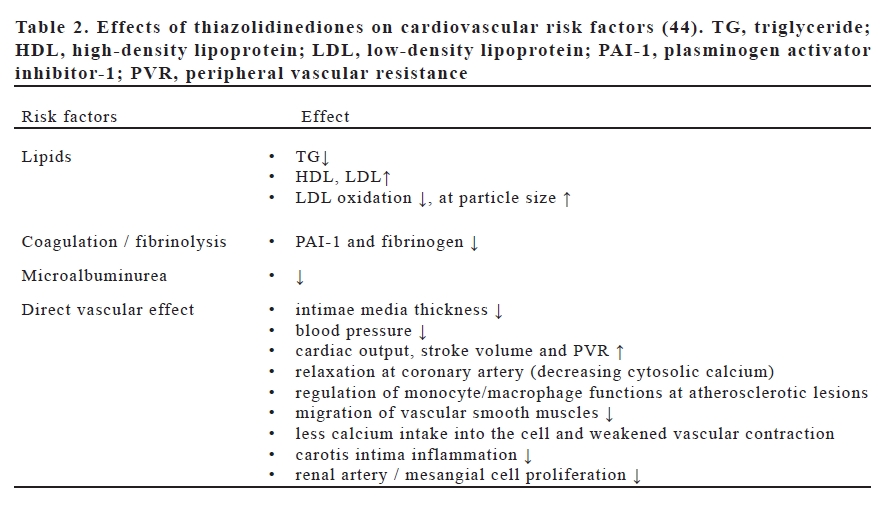
Cardiac and vascular sulfonylurea receptors are naturally different from the pancreatic receptors (34). Being a second generation sulfonylureas, glimepiride is much more specific to pancreas and does not show any interaction with cardiovascular ATPdependent potassium channels (40). Meglitinids Like sulfonylureas, they interact closing of the ATP-dependent potassium channels; however, their interaction mechanism is much more complex. They decrease both fasting glucose level and the HbA1c, but do not show a significant effect on lipid profile. They have some specific characteristics to distinguish them from sulfonylureas; 1) they are taken before the meals (not taken in case a meal is neglected), 2) they exhibit short-term effects and are of short pharmacological half life, 3) they mainly affect on the level of postprandial glucose. At the end of one-year follow-up, an increase was observed in morbidity (especially in acute ischemic events) in those taking repaglinide compared with glibenclamide (41). The present data, however, are not enough so as to make a decision on the CV reliability of these drugs. When the effect mechanisms are taken into consideration, it is necessary to administer them very carefully. Glitazons (Tiazolidinedions) Their chemical structures and effect mechanisms are different from those of the other groups. They are insulin sensitizers similar to metformin. They increase the sensitivity to insulin, especially in the cells of fat, muscle and cardiovascular system. Due to its hepatoxicity, troglitazone, the first agent of this class has been banned from clinical use in the USA, but afterwards the studies done with rosiglitazone and pioglitazone have established that hepatotoxicity is not a class effect (45). Glitazones lead to increased glucose transporter expression by binding to nuclear “peroxisome proliferator-activated receptor (PPAR) γ”. They also improves sensitivity to insulin particularly in adipocytes, muscle and liver, and a suplementary effect is the inhibition of hepatic gluconeogenesis (42). Glitazons do not increase insulin secretion. PPARs are the transcription factors belonging to nuclear receptors family. There are 3 known isoforms; α, β/δ, γ. These receptors regulate glucose balance, lipoprotein metabolism, local immune response, local inflammation, tumor development and thrombosis. Moreover, they have potential antiatherogenic effects (43). Tiazolidinedions contribute to the improvement of the endothelial functions with various mechanisms (with the effects on nitric oxide synthesis, PPAR-γ receptors and various cytokines). Meanwhile, they may prevent the progression of atherosclerosis inhibiting “monocyte chemo-attractant protein-1” release in the endothelial cells. Glitazones having an evident antiinflammatory and antioxidant characteristics supress the inflammatory mediators and weaken the response of the endothelial cells to TNF-α (44). Glitazones moderately decrease the glucose and HbAlc levels. They decrease the plasma TG level up to 10 to 20% stimulating PPAR-α, and also increase the HDL level up to 5 to 10%. Although these positive effects are stated to be balanced with the increase of LDL level up to 5 to 10% (45), the increase of larger LDL particles being less atherogenic is dominant. However, the small intensive LDL particles being more atherogenic and playing a basic role in the development of atherosclerosis are demonstrated to decrease with the thiazolidinedion treatment (44). The last findings have indicated that rosiglitazone decreases excretion of urinary albumin in type 2 DM and even may decrease the blood pressure slightly (46). This effect of glitazones, the blood pressure decreasing effects of which were established in various studies is to be linked to the following; 1) glitazones increase insulin-mediated vasodilation raising insulin sensitivity, 2) they inhibit intracellular calcium and myocyte contractility, 3) they inhibit endothelium-1 secretion (44). In type 2 DM, a decrease in vascular intimamedia thickness was observed with glitazone treatment. It has also been established that they inhibit the secretion and the function of “matrix metalloproteinase-9” contributing to the plaque rupture process in acute coronary events. In addition, glitazones have been shown to decrease the levels of CRP, IL-6 and leukocytes in some studies (44). Glitazones may lead to weight gain at different levels in relation to the decrease of the levels of the leptin in proportion to the dose taken (47). However, a decrease of the intraabdominal fat mass was shown, whereas there is no evident change at the body weight with the use of glitazones (44); that is, glitazones have been shown to change body-fat distribution positively and thus may reduce the cardiovascular risk . As each of the drugs in this group is metabolized through different cytochrome pathways (CYP), there are differences in the drug interactions. Even though rosiglitazone mainly uses CYP 2C8, pioglitazone uses CYP 3A4 and CYP 2C8. When considering that CYP 3A4 is used in the metabolisms of more than 150 drugs, the drug interaction with pioglitazone can be estimated further. Glitazones lead to a slight decrease in hemoglobin and hematocrit as the consequence of hemodulition as a class effect. In 5 percent of the patients, edema has been reported and thus, glitazones are contraindicated in NYHA class III-IV patients (45). Consequently, glitazones have beneficial effect on a great scale, but also harmful cardiovascular effects to some extent (Table 2). Due to their many positive effects, they inspire hope although further clinical studies are needed to decide on their cardiovascular reliability. α-Glucosidase inhibitors The basic effect mechanisms of these drugs are the competitive inhibition of some α-glucosidase group enzymes such as maltase, isomaltase, sucrase and glucoamylase. These enzymes are the ones bound to the membrane in the brush border of the small intestine and hydrolyze oligosaccharides and disaccharides to glucose. By delaying the digestion of carbohydrates, they cause the absorption of carbohydrates to occur in more distal small intestine and colon. They have less hypoglisemic potentials than biguanids and sulfonylureas. Their most common side effects are mild abdominal pain, gas and diarrhea (45). It has been known that the impaired fasting glucose cocentration is a poorer sign of prognosis in nondiabetic patients with ischemic heart disease (48). In these patients, acarbose can be used as an addition or an alternative to the change of life style to delay the development of type 2 DM (49). In long term, the effects of these drugs on diabetic micro-and macrovascular complications and on morbidity and mortality rates are not known yet (50). Combined Antihyperglycemic Treatment In United Kingdom Prospective Diabetes Study (UKPDS), glucose levels were detected to be at appropriate levels in about 50 percent of this patients at the end of 3 years and in only 25 percent of them at the end of 9 years through monotherapy (51). For this reason, a significant number of the patients require a combined antidiabetic treatment. This treatment has not yet been proved to be effective in preventing or delaying macrovascular disease although the combination therapy is known to control glucose level better. In UKPDS, it has been detected that the mortality rate depending on all reasons is increased in all diabetic populations taking the combined treatment (especially in those taking metformin at early stage) (21). Data accumulated through studies have shown that the combination of metformin and sulfonylurea (especially glibenclamide) increases the mortality rate including all reasons at the end of average 7.7 years in diabetics with CAD (52). In another study, the combination of sulfonylurea and metformin has been established to cause a higher cardiovascular mortality rate in the patients with type 2 DM compared to the ones taking only sulfonylurea (53). Combined antihyperglycemic treatment still keeping as a special problem due to the fact that sulfonylureas and metformin are the most effective antidiabetic drugs, have the most adverse cardiac effects and have most commonly been combined in clinical practice. Clinical Implications It is generally very difficult to choose the best treatment among so many drugs and in the presence of CAD, this becomes more difficult. It is essential in all patients to decrease the risk factors effectively such as diet, physical activity, quitting cigarette smoking, weight control, treatment of hypertension and hyperlipidemia. Maintenance of glucose levels at a normal or close to normal points with pharmacological agents in long-term is known to decrease the morbidity and mortality rates by generating positive effects on microvascular diseases such as retinopathy, nephropathy and neuropathy (54). Yet, it is difficult to express the same for CAD when thinking about the adverse cardiovascular effects of most antidiabetics at various levels. During the 3-month period after acute myocardial infarction, glycemic control with insulin increases survival rate, and the benefits of an alternative treatment is not certain yet. Metformin or sulfonylurea can be considered as a first choice in the obese patients with CAD as well as type 2 DM. However, concomittant use of glibenclamide and metformin should be avoided. No satisfactory data is avaliable on the combination of metformin with other sulfonylureas. A glucosidase inhibitor and finally insulin can be added by taking the risk of hyperinsulinemic hypoalphalipoproteinemia into account (especially in case of low HDL cholesterol level) unless sufficient glucose level control can be provided (45). Insulin-sensitizer agents may decrease myocardial infarction incidence and protect myocardium. Metformin has been shown to decrease myocardial infarction and mortality risk after PCI. However, in another study in which biguanide and/or thiazolidinedione therapy (insulin-sensitizer) were compared with insulin and/or sulfonylurea treatment (insulin-providing) as hypoglicemic treatment after acute coronary syndrome, 90day mortality rate, myocardial infarction and severely recurring ischemia have been found to be higher in the insulin-provided group (55). It is also of vital importance to decide optimal antidiabetic treatment as well as the for optimal treatment of CAD in these patients because of the increased cardiovascular mortality rate among diabetic patients. Therefore, well-designed, randomized and further clinical studies are needed. As mentioned previously, glitazones have many positive cardiovascular effects, and so they inspire hope for the diabetics with CAD. REFERENCES
Copyright 2007 - European Journal of General Medicine The following images related to this document are available:Photo images[gm07044t2.jpg] [gm07044t1.jpg] |
| |||||||||

{kind=link}