 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
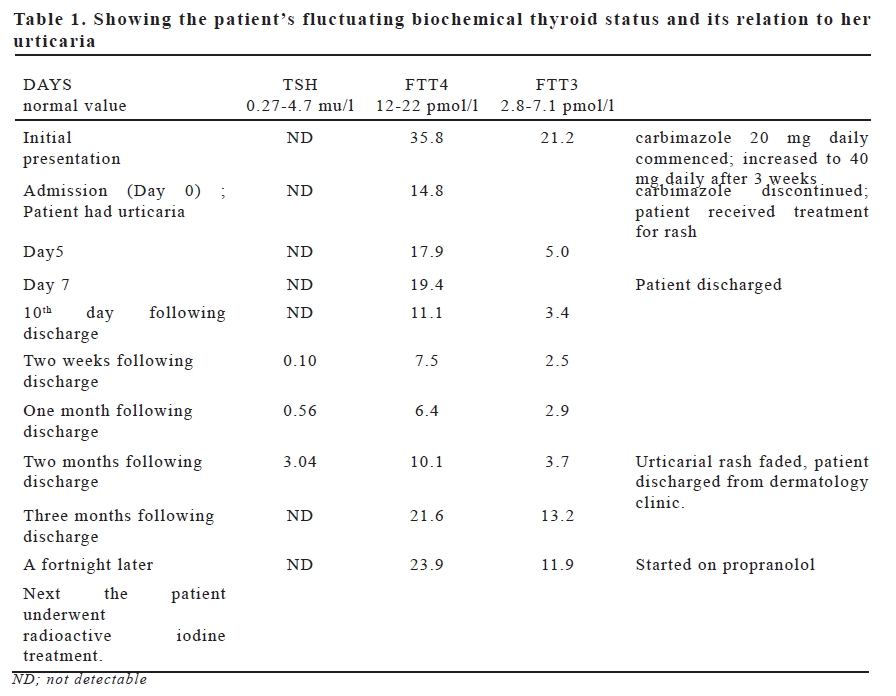
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 205-208 Case Report Urticaria - An Uncommon Presentation Of Thyrotoxicosis Indrajit Talapatra, Karthik Prabhakar , David James Tymms Royal Albert Edward Infirmary, Diabetes Centre, Department of Medicine, Wigan UK Code Number: gm07047 We describe below two patients who presented with thyrotoxicosis and were put on carbimazole treatment. Both of them developed urticarial rash following commencement of carbimazole treatment. The drug was stopped but the patients continued to have the rash for a few months. One patient became biochemically hypothyroid despite cessation of treatment but again became biochemically and clinically hyperthyroid and subsequently underwent radioactive iodine treatment. The other patient was treated with propylthiouracil and became euthyroid. It was found that the urticaria improved in both patients as their overactive thyroid status got better. Key words: Thyrotoxicosis, urticaria, carbimazole, propylthiouracil INTRODUCTION Uticaria can be autoimmune in aetiology and when it persists for more than six weeks it becomes chronic in nature. Urticaria can develop with auto immune thyroid disorder and persist for more than six weeks. In thyrotoxicosis patient receives treatment with carbimazole or propylthiouracil and while on treatment may develop the rash of urticaria. The antithyroid drug is therefore discontinued, considering the rash to be drug induced. However it is not until the overactive thyroid status improves or the patient becomes euthyroid that the rash fades out. CASE 1 The first patient was a 25 year old woman who presented with weight loss, tremor and mood swings. She was biochemically thyrotoxic. Her investigation results showed TSH (Thyroid stimulating hormone) was not detectable (normal: 0.27-4.7 mu/l), FT4 (Free thyroxine) 35.8 pmol/l (normal: 1222) and FT3 (Free triiodothyronine) 21.2 pmol/l (normal: 2.8-7.1). Her TPA (Thyroid peroxidase autoantibody) was 67 ku/l (normal: 0-34). She had a moderate size goitre. Technetium Partechnetate, 40 mBq scan showed uniform heavily increased isotope uptake (7.3% at 20 mins). There was a large cold area in the upper half of left lobe. She was commenced on carbimazole 20 mg daily which was increased to 40 mg daily after three weeks. An ultrasound of thyroid showed that the right lobe of thyroid was much larger with nodularity of parenchyma and the left lobe was smaller ( Right lobe measured 1.4cm x 1.1cm x 3.9 cm and the left lobe measured 0.9cm x 0.7 cm x 3.3cm). The patient next presented with an itchy red maculopapular rash 10 days following increase of dose of carbimazole treatment but it had started earlier, while she was still having the symptoms of overactive thyroid. The rash was on the face, trunk and dorsal aspect of the extremities. She was admitted. Her blood results showed TSH was not detectable and FT4 14.8 pmol/l. Her carbimazole was discontinued and she was commenced on intravenous hydrocortisone and chlorpheniramine. She was seen by a dermatologist and was diagnosed to be having urticaria. Her subsequent medications included prednisolone 40 mg daily (with the idea of reducing the dose by 10 mg every 7 days), hydroxyzine 25 mg at night, chlorpheniramine 4 mg four times daily, fexofenadine 180 mg daily and Balneum cream (containing urea) topically. The patient’s thyroid status continued to remain biochemically stable and she was discharged after a week. Her FT4 became slightly low 10 days following discharge and continued to remain so for more than 2 months. The patient’s urticatial rash persisted despite having come off carbimazole but gradually she was able to come off steroids and antihistaminics 2 months following her discharge from the hospital. Her rash had faded and she was discharged from dermatology follow up. While the patient was biochemically mildly hypothyroid she underwent a technetium uptake scan of thyroid which showed normal uptake into the right lobe of thyroid (2.36% at 20 minutes) and the left lobe was much smaller. Next the patient again became biochemically thyrotoxic with TSH not detectable, FT4 23.9 pmol/l and FT3 11.9 pmol/l. and a technetium scan showed increased uptake of 5.08% at 20 minutes. The patient was commenced on propranolol 80 mg daily and subsequently underwent radioactive iodine treatment (400 mBq) and is currently under close follow up of the endocrine clinic. There has been no recurrence of the rash. The patient possibly had Graves’ disease with fluctuating thyroid status, depending on the level of TSH receptor stimulating or blocking antibody. CASE 2 The second patient was a 44 year old woman who presented to her general practitioner with tremor, palpitation , weight loss, a small size goitre and proptosis and was diagnosed to be thyrotoxic. Her TSH was not detectable, FT4 was 48.2 pmol/l and FT3 was 29.3 pmol/l. Blood test results a week later showed her TSH to be not detectable, FT4 was 50.5 pmol/l. The patient was commenced on carbimazole 40 mg and propranolol 80 mg daily. Two months later her investigation results showed TSH not detectable, FT4 8.6 pmol/l and FT3 4.4 pmol/l. Her TPA was 477 ku/l. Her carbimazole dose was reduced to 10 mg daily. A month later the patient developed an itchy pink maculopapular rash over the trunk and extremities. Suspecting it to be a drug rash her carbimazole and propranolol were discontinued. The rash continued to persist. A month later the patient presented to the endocrine clinic when she was clinically and biochemically thyrotoxic and had the itchy rash which persisted despite having come off carbimazole and propranolol. The rash was thought to be urticaria and later confirmed so by a dermatologist. Her TSH was not detectable, FT4 41.8 pmol/l and FT3 17.9 pmol/l. Tecnetium uptake scan suggested Graves’ disease. The patient was commenced on propylthiouracil 200 mg daily and 6 weeks later her investigation results showed her TSH was not detectable, FT4 10.8 pmol/l and FT3 4.6 pmol/l. Her urticarial rash had faded with improvement of her thyroid status. Her propylthiouracil dose was reduced to 100 mg daily. Table 2. Summarizing the 2nd patient’s biochemical thyroid status and its relationship to urticaria
DISCUSSION Urticaria and pruritus are rare skin manifestations of thyrotoxicosis (1,2).The urticaria responds poorly to antihistaminics and partially to systemic steroids, but resolves when the thyroxine level is reduced to normal (3). In both of our patients the urticarial rash improved as the patients’ thyrotoxic status got better. The exact mechanism of urticaria in thyrotoxicosis is unknown but thyroxine may increase modulation of cyclic AMP levels within the mast cells (1,3). It is possible that a cross-linking of IgE receptors of mast cells induced by antithyroid antibodies may be a cause of histamine release (4). Urticaria has also been reported in Hashimoto’s thyroiditis (4,5). Recent studies have shown a 10-20% prevalence of antithyroid antibodies in the sera of patients with chronic idiopathic urticaria. In a recent study(6) 23% prevalence of antithyroid antibodies were found in the sera of patients with chronic idiopathic urticaria and 33% in sera of patients with urticaria of known aetiology.Evidence of thyroid dysfunction was found in about 40% of patients with antithyroid antibodies and urticaria (both groups). Carbimazole was discontinued in both of our patients with the development of rash, thinking it to be drug induced. However the rash persisted despite cessation of carbimazole treatment. It was only when the patients recovered from thyrotoxicosis that the urticarial rash faded. In the second patient there was no recurrence of rash despite continuing treatment with propylthiouracil. In conclusion, urticaria is an uncommon manifestation of thyrotoxicosis. However it can present during any stage of the disease and may lead to the misdiagnosis of anti thyroid drug induced rash. On the contrary if the thyroid status improves with treatment, urticarial rash gets better. REFERENCES
Copyright 2007 - European Journal of General Medicine The following images related to this document are available:Photo images[gm07047t2.jpg] [gm07047t1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}