 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 209-212 Case Report A Case Of Brucellosis Lymphadenitis Mimicking Scrofuloderma Hasan Karsen1, Mustafa Kasım Karahocagil2, Hayrettin Akdeniz2, Mahmut Sünnetçioğlu2, Ömer Evirgen3 Hakkari State Hospital, Department of Infectious Diseases and Clinical Microbiology1,
Hakkari, Yüzüncü Yıl University Faculty of Medicine, Department of Infectious Diseases and
Clinical Microbiology2, Van, Adıyaman State Hospital, Department of Infectious Diseases and
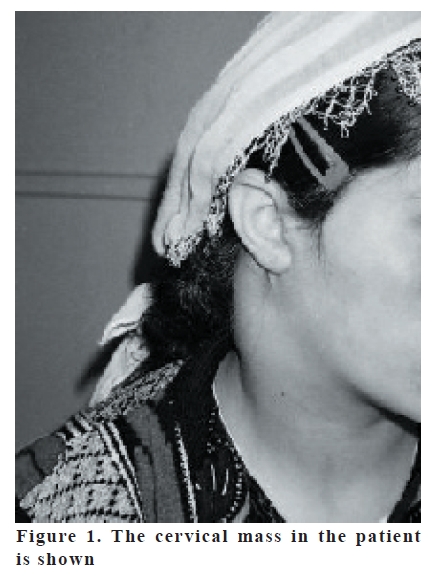
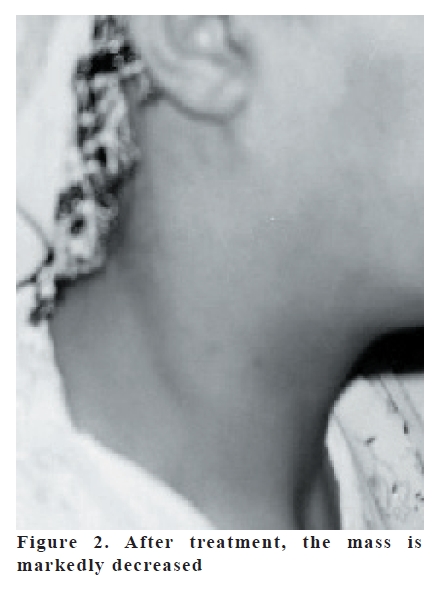
Clinical Microbiology3, Adıyaman, Turkey Code Number: gm07048 Brucellosis is a zoonotic disease, which may be manifested by multisystemic involvement. While the complications related to musculoskeletal and gastrointestinal system are frequently seen, those related to the other systems are rarely encountered. In this paper, we present a brucellosis lymphadenitis case in the right side of the neck in a 20 years old female patient, presenting with a mass formation in the soft tissue mimicking scrofuloderma, with dimensions of 10x6x4 cm. Especially in endemic areas, brucellosis lymphadenitis should also be remembered in addition to scrofuloderma Key words: Brucellosis; lymphadenitis; scrofuloderma; subcutaneous mass INTRODUCTION Brucellosis is still an important health problem in developing countries, especially among people living in rural areas dealing with stock-breeding (1,2). Many manifestations such as hematopoetic, endocrine, cardiovascular, gastrointestinal, genitourinary, musculoskeletal, ocular, respiratory, neuropsychiatric, skin and soft tissue involvement may be seen during the course of the disease (3). In this paper, a brucellosis case presenting with cervical lymphadenitis is presented. As far as we know, such a case of brucellosis lymphadenitis mimicking scrofuloderma has not been reported in the literature. CASE A 20 years old female patient dealing with stock-breeding with her family attended to our department with complaints of a swelling on her right cervical region and right shoulder pain. Prior to admission, complaints of fever, sweating and backache had begun 15 months ago. Three months later, a swelling on the neck and bilateral knee swelling were noted. She was admitted to the Department of Internal Medicine with these complaints. She was told to be brucellosis and probably given rifampicin and doxycycline, but she used these drugs only 1 month. The swelling in her right neck partly decreased after 1 month of using these drugs, the knee joint swelling disappeared and the other complaints subsided. Afterwards namely one year later, a combined treatment of rifampicin, doxycycline and ciprofloxacin was given to the patient when she was admitted to the Department of Infectious Diseases because of the increase of the swelling on her neck. After 2 weeks of treatment, thereupon her complaints persisted; the patient was referred to the Department of Otorhinolaringology with the preliminary diagnosis of scrofuloderma. Since the brucella standard agglutination test (SAT) resulted positive at titer of 1/320 in serum, the patient was re-admitted to our department and hospitalized. Brucella SAT was positive at titer of 1/320 in the fluid taken with fine needle aspiration from the patient’s mass. The mass was accepted as a brucellosis-associated mass, thus the combined treatment consisting of ceftriaxone (4 g/day intravenous), rifampicin (600 mg/ day, per oral) and doxycycline (200 mg/day per oral) was started together with naproxene sodium. There was a history of consumption of fresh cheese made from raw milk and their animals have aborted many times. On physical examination: blood pressure was 130/90 mmHg, pulse rate 80/min, axillary temperature 36.5 º C, breathing rate 20/min. The mass was stiff in nature, in same color with the skin, superficial, with clear margins, painful, attached to the skin, in dimensions of 10x6x4 cm which was extending from the right mandibular corner to the clavicula (Figure 1). The examination of the other systems revealed no pathology. On laboratory investigations, leukocyte count was 7750/ mm3 (with differential of neutrophils 62%, lymphocytes 23%, and monocytes 11%); hemoglobin 9.4 g/dL; platelet count 220.000/mm3; erythrocyte sedimentation rate 30 mm/h; C-reactive protein <3.25 mg/ L; fasting blood sugar 81 mg/dL; alanine aminotransferase 48 U/L; and alanine serum transferase 58 U/L. The other biochemical parameters were normal. Additionally, tests for tuberculin, human immunodeficiency virus, toxoplasmosis, typhoid fever and syphilis were negative; the chest radiography was evaluated as normal. Gram, Ehrlich-Ziehl-Neelsen (EZN) and fungal stains of the mass fluid were unremarkable. No bacterial and fungal growth occurred in the cultures performed from the blood and the mass fluid. Histopathological examination of the mass fluid revealed benign reactive lymphadenitis. On the ultrasonography of her neck which was performed on the second day of hospitalization, multiple conglomerated lymphadenopathy was observed. This mass was extending from the right mandibular corner to the inferior, the largest one being with dimension of 24x12 mm. Because the patient did not accept the surgical operation and the mass size decreased approximately at a rate of 50% on the 30th day of treatment, ceftriaxone was stopped and the patient was discharged from the hospital to come to the control follow-up with one month intervals. Brucellosis treatment with rifampicin and doxycycline was maintained for additional 5 months. During her follow up, the laboratory investigations returned to normal and the mass markedly disappeared (Figure 2). DISCUSSION Brucellosis is a zoonotic disease, which can be seen worldwide (4). It is widespread especially in Eastern and South-Eastern Anatolia regions of our country (5). Transmission to human generally occurs by gastrointestinal route, then the bacteria enter the lymphatics and replicate within regional lymph nodes. Hematogenous dissemination is then followed by localization of bacteria within organs rich in elements of reticuloendothelial system, such as liver, spleen and bone marrow. While the complications related to the musculoskeletal and gastrointestinal systems are frequently seen, complications related to the skin and soft tissue are rarely encountered (6). Nine cases of brucellosis–associated soft tissue abscesses have been reported from 1968 onwards up to date in the literature (7). Skin and soft tissue manifestations of brucellosis are generally accompanied by general symptoms of brucellosis (4). Also in our case, general symptoms of brucellosis had been continuing for 3 months before the development of the cervical mass. Since the clinical symptoms of brucellosis are quite similar to the other infectious and noninfectious diseases, many diseases should be taken into consideration in differential diagnosis. (8). Among them may be cited acute bacterial infections of the lymph nodes, plague, tularemia, actinomycosis, fungal infections, cat scratch disease, infectious mononucleosis, toxoplasmosis, scrofuloderma and malignity (9). Despite the fact that our patient was young, the complaints such as fever, backache and loss of appetite had been continuing for 15 months. This firstly made us consider that the case may be scrofuloderma or a malignity. Since there was no fistula and caseification necrosis on her physical examination, and EZN staining was negative in the fluid obtained by fine needle aspiration together with a positive SAT result at titer of 1/320 in this fluid, the diagnosis of scrofuloderma was ruled. There was no other finding indicating tuberculosis such as positive tuberculin test and/or chest radiography in the patient either. The long duration of the disease was attributed to the early discontinuation of antibrucellar drugs by the patient herself. Because the histopathological examination of the mass fluid was evaluated as benign reactive lymphadenitis, the case was accepted with the present findings as brucellosis lymphadenitis mimicking scrofuloderma. Since the patients use frequently various antibiotics before the diagnosis was achieved, as in our case, and the growth of the agent is quite late in the culture media, the diagnosis of brucellosis is widely done by serological methods (10). Taking into account that brucellosis can result in miscellaneous complications, as seen also in our case, it should be considered in differential diagnosis of soft tissue masses and the diagnosis should be achieved either by culture or by serological methods. Treatment duration must be at least 6 weeks and in the presence of any complication, the treatment duration and combination should properly be lengthened according to the clinical and laboratory findings (6). Because the treatment duration is quite long in brucellosis, adaptability of the patients to the treatment is as important as the treatment itself. In our patient, triple antibrucellar treatment with rifampicin, doxycycline and ciprofloxacin was started at our outpatient clinic, but upon hospitalization after histopathological diagnosis was achieved, ceftriaxone was replaced by ciprofloxacin and maintained for 1 month with rifampicin and doxycycline that was maintained for additional 5 months. In conclusion especially in endemic areas, in differential diagnosis of subcutaneous masses resisting to the treatment with chronic course, brucellosis should also be remembered along with scrofuloderma. As far as we know, because such a case of brucella lymphadenitis mimicking scrofuloderma has not been reported in the literature, we think that similar to the definition of scrofuloderma for tuberculosis presenting with lymphadenitis in the cervical area, a new entity and probably a peculiar name could be given to that presentation of brucellosis presenting with lymphadenitis in the same area. REFERENCES
Copyright 2007 - European Journal of General Medicine The following images related to this document are available:Photo images[gm07048f1.jpg] [gm07048f2.jpg] |
| |||||||||

{kind=link}
{kind=link}