 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
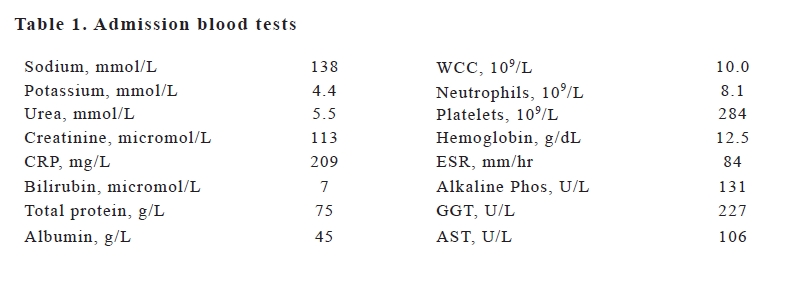
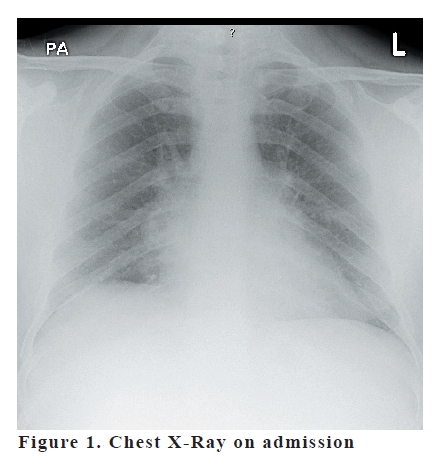
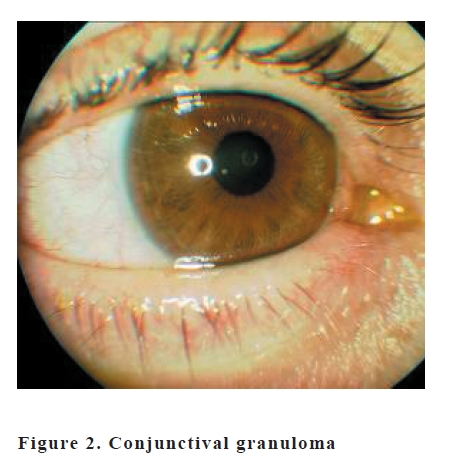
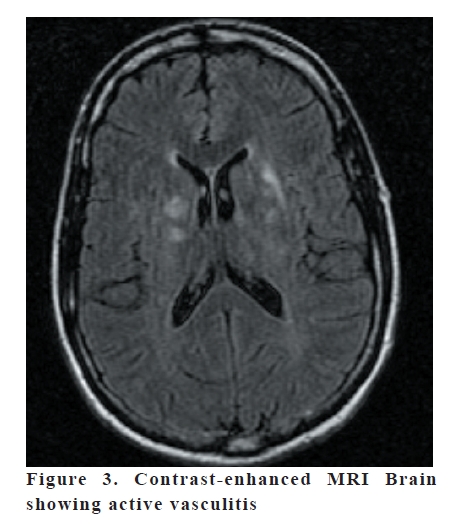
European Journal of General Medicine, Vol. 5, No. 4, 2008, pp. 213-216 Case Report A Young Man With Iritis, Nephritis And Hepatitis Anuroop Gogi, Katherine Foley Princess Royal University Hospital, Farnborough, UK Code Number: gm07049 The association between sarcoidosis and vasculitis is not well documented in literature. This case report is one of the rare instances where both occur together. However the significance of this still needs to be understood. Vasculitis as a result of granulomatous inflammation caused by sarcoid has been documented where no other cause of vasculitis can be found. Key words: Sarcoidosis, vasculitis, nephritis, hepatitis INTRODUCTION A 38 year old gentleman presented to the Princess Royal University Hospital in Bromley with swinging fevers and red eyes. Mr PG, a white Caucasian male came in with a 2 week history of lethargy, night sweats, reduced appetite and a non-productive cough. He was also complaining of pains in both his knees and his right wrist. Four days prior to his coming to hospital, he started feeling breathless unrelated to exertion and developed a red non-itchy rash over his face and neck. His past medical history was unremarkable. He had never been out of the country and did not have contact with TB. He did not have any urinary symptoms and his bowel movements were fine. He was married with a 6 year old healthy son and smoked about 10 cigarettes a day for 20 years. He also drank between 30 and 40 units of alcohol in a week. He was a plumber by profession and had a vague history of contact with sewage 2 weeks previously. The patient also denied high risk sexual activity, IV drug abuse, needle stick injury or any blood transfusions in the past. On examination, he looked unwell and had a temperature of 38°C. He had injected conjunctivae bilaterally and an erythematous petechial non-blanching rash over his face and hands. There was no lymphadenopathy and he was not jaundiced or pale. His JVP was not raised and blood pressure was 120/70. Heart rate was 80 per minute and heart sounds were normal. Chest was clear and abdomen examination showed a 2 cm smooth hepatomagaly with normal bowel sounds. The neurological examination was normal with downgoing plantars and normal reflexes. ECG showed Sinus rhythm at a rate of 80/ min and left axis deviation. The provisional diagnosis at that time was an atypical pneumonia, Sarcoidosis and Leptospirosis. He was started on IV Benzyl Penicillin and Clarithromycin and admitted, pending further investigations. The initial tests were negative for atypical Pneumonia and Glandular fever. An Ultrasound of his abdomen showed smooth hepatosplenomegaly with normal kidneys, urinary bladder, Gall bladder, biliary ducts and no ascites. Meanwhile, he was seen by a consultant ophthalmologist who noted bilateral conjunctival granulomas which were biopsied. The impression was that of a bilateral granulomatous uveitis with iris nodules and a differential of Sarcoid, TB and Syphilis was offered. He was also started on topical steroids and mydriatics and the redness in his eyes responded to these and disappeared over a week. The serum ACE level was normal at 46 Units/L and the adjusted Calcium was 2.18, Phosphate 1.10. Alkaline Phosphatase initially increased to 300 and then slowly normalised over the course of the next two weeks. The renal function followed a similar pattern with Creatinine initially rising to 140 and then normalising over the next two weeks. The inflammatory markers remained high with ESR around 120 and CRP at 70. All autoantibodies including Anti-nuclear and ANCA were negative. The blood and urine cultures were negative for pathogens. The hepatitis antibodies and Leptospira antibodies were negative. Conjunctival biopsy showed scattered submucosal aggregates of epitheioid macrophages with occasional giant cells and no evidence of caseation. AAFB staining was negative. The impression was that of noncaseating granulomatous inflammation. A renal biopsy was considered but not done as his renal function had improved by then. He improved clinically and biochemically over two weeks and was then discharged with a plan to get a Gadolinium enhanced MRI of his brain in view of the conjunctival, hepatic and renal abnormalities. The patient was readmitted to hospital about 3 months later. He had come in for an MRI as out-patient when he suddenly developed weakness and numbness of the left side of his body, left facial droop and dysarthria. The symptoms and signs improved over the next 2 days after starting treatment with Gluco-corticoids and a neurological examination the next day WCC, 109/L 10.0 Neutrophils, 109/L 8.1 Platelets, 109/L 284 Hemoglobin, g/dL 12.5 ESR, mm/hr 84 Alkaline Phos, U/L 131 GGT, U/L 227 AST, U/L 106 was normal, with flexor plantars and normal reflexes and power. An enhanced MRI scan of brain with an MR Angiogram was carried out as planned. The scan showed multiple abnormal high signal areas in the brain stem, right cerebellar peduncle, both thalami, both lentiform nuclei, both caudate nuclei extending into the corona radiata and right cerebellar hemisphere. Following intravenous Gadolinium, there was enhancement of the lesion in the right cerebellum, right globus pallidus and right corona radiate with rim enhancement of the lesion in left caudate nucleus. The appearances were those of an active cerebral vasculitis. Taking into consideration his clinical history, a differential of Behcet’s was offered although its well-known that Behcet’s is extremely rare in white Caucasians. The appearances were atypical for Neuro-sarcoidosis. A Lumbar Puncture showed white cell count of 25/cmm, 95 % of them being lymphocytes. Protein content was 0.4 and Glucose was 3.5, plasma glucose being 5.5. A whole body Gallium scan showed slightly increased uptake in the salivary glands and small nodular uptake in the lungs bilaterally. Figure 1, Figure 2 and Figure 3 DISCUSSION Behcet’s can safely be ruled out in this patient. It is extremely rare in white Caucasian males; Pathergy is very hard to miss ( especially with the number of blood tests these patients have ); At least 3 episodes of oral ulceration in a 12 month period are needed for the dignosis of Behcet’s ( as per guidelines by the International Behcet study group); Arthritis in Behcet’s usually affects the knees and spine; Skin manifestations usually are in the form of Erythema nodosum and papulo-pustular acneiform lesions. Tuberculosis, although a possibility, is very unlikely. This man presented with a pneumonic illness initially which seemed to get better over 3 weeks. Non-caseating granulomas may be seen in TB but in a relatively young white male who has never been out of Britain and has not had contact with it, TB can affect only if he is severely immuno-compromised. He was fairly well between the two admissions. Even though such an aggressive form of Neuro-sarcoidosis with a relative paucity of pulmonary manifestations is very rare,the most likely diagnosis in this man is probably still Sarcoidosis. The chest X-Ray in this article and all his subsequent X-Rays just showed pneumonic consolidation in the right middle lobe without hilar lymphadenopathy or pulmonary infiltrates. His serum ACE and Calcium were normal throughout the course of his illness. However, aggressive forms of sarcoid affecting mainly the lungs, eyes, parotids and the meninges have been noted before. This man’s iritis settled almost instantly with steroids. The second admission was for a transient ischemic attack which did not require treatment. Vasculitis is not traditionally a part of Sarcoid, although in this man, vasculitis would certainly explain a lot of things- the rash, the fever, the markedly abnormal inflammatory markers with normal white cell count, renal impairment, neurological symptoms and the MRI findings. The conjunctival granulomas and hepatosplenomegaly are more a manifestation of Sarcoidosis. This is most probably Sarcoid Vasculitis, a very much under-appreciated and rare appearance of sarcoid disease. There have been 14 studied cases of Sarcoid vasculitis in USA and 8 in UK till 2000. There have been a few case reports linking sarcoid and vasculitis in the past. Our patient differs from them in a few important aspects: In all patients except one, sarcoid disease manifested many years before the onset of vasculitis; In our patient, the time gap was 3 months.It was noted in the United States that white patients tended to develop both small and large vessel vasculitis and black patients, large vessel vasculitis; Our patient is white and manifested disease only of small vessels There were also prominent similarities- Response to Gluco-corticoids; Presence of uveitis ( 50% of previous patients with sarcoid vasculitis had uveitis) ; Renal impairment; Neurological signs. In conclusion, vasculitis seems to be a part of a particularly aggressive form of Sarcoid disease. Even though the actual number of patients with sarcoidosis who manifest vasculitis is small, when it does occur, it causes multiple organ involvement and morbidity. The aetiology of Sarcoidosis is unknown at present. Vasculitis, in comparison, is much more studied and documented. There are a wide variety of immuno-inflammatory changes recognised in specific forms of vasculitis such as Takayasu’s. The association between Sarcoidosis and vasculitis seems to be more than co-incidental since both of them are really rare. More case reports linking sarcoid and vasculitis may lend credibility to the theory that sarcoidosis is an inflammatory disease. REFERENCES
Copyright 2007 - European Journal of General Medicine The following images related to this document are available:Photo images[gm07049f2.jpg] [gm07049t1.jpg] [gm07049f1.jpg] [gm07049f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}