 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 4, No. 4, 2008, pp. 217-218 BRIEF REPORT Is Skin Nourishment Always Possible Through The Perforators In A Musculocutaneous Flap? Adem Özkan, Zekeriya Tosun, Nedim Savacı Selcuk University Meram Medical Faculty, Plastic and Reconstructive Surgery Department,
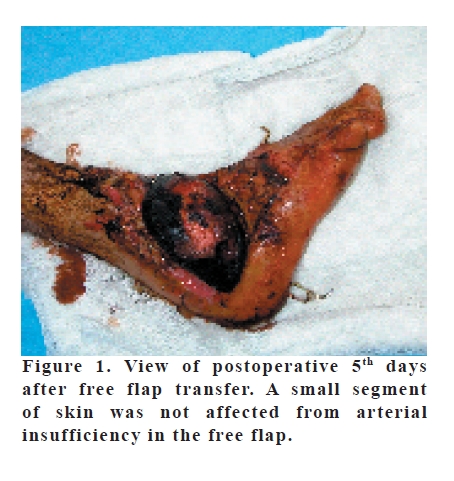
Konya, Turkey Code Number: gm07050 We present a case with vertical rectus abdominis myocutaneous free flap in which deep inferior epigastric perforators does not nourish skin paddle of the flap. The skin paddle of musclocutaneous flaps is nourished by musculocutaneous perforators originating from the main vascular system of the muscle. The skin paddle of rectus abdominis flap is also supplied by musculocutaneous perforators of deep inferior epigastric artery (1). Cutaneous perforators end directly within the skin. Their origin may be either from the source artery or from the subcutaneous or fascial brances (2). Twenty-year-old man who had soft tissue defect with exposed bone tissue on the lateral surface of the ankle due to traffic accident admitted to our clinic. Using vertical rectus abdominis myocutaneous free flap, closure of exposed bone tissue defect was planned. The flap was raised for microvascular transplantation based on elevation of the standart technique by using 4x magnification surgical loop. We initially observed that capillary refill of the flap was delayed under the tension-free condition of the perforators. Then, circulation of flap spontaneously and completely returned to normal. The pedicle was re-explorated due to ischemia after postoperative 50 hours. No causing agent, such as thrombosis or techniqual problem existed either in the artery or in the vein. We applied vasodilator agent (lidocain) on arterial anastomosis for assesment of vasospasm, but there was no vasodilatation. Therefore, we think that there was no vasospasm. Almost all of the skin was affected from arterial insufficiency (Figure 1). However, muscle and fascia’s circulation were normal (Figure 2). Thus, after a period of week wound care, the defect was closed with split thickness skin graft. In our patient, although all surgical tecniques and medical supports are sufficient, the absence of nourishment of the skin paddle may be explained in two way: first, direct cutaneous vessels may be more important than the musculocutaneous perforators for abdominal skin circulation. Survival of skin above the central of flap was supported our idea. Second, conventional acoustic Doppler cannot provide sufficient information about musculocutaneous perforators. Conventional acoustic Doppler sound can only provide more trusted information about the position of penetrating points of the perforating vessels through the fascia. But it cannot provide information about whether the vessel runs above or below the fascia for a few centimeters (2). Indeed, we found three perforators by using conventional acoustic Doppler for our case. There are many different vascular patterns in the deep inferior epigastric perforators that run up and down the rectus muscle. Yano et al. (3) found that dominant perforator did not run into the muscle in their case. Blondeel et al. (2) also reported two patients who had a total of three perforators turning around the edge of the rectus abdominis muscle. However, the perforators in our flap were penetrating posterior surface of the rectus abdominis muscle. As defined a rule “all or none” in free flaps is not enough to explain the situation. Because there were no vasospasm, thrombosis or technical problem in our pedicle, we think that insufficient perforator vessels are only reason leading to ischemia in our flap. Accordingly, we suggested that musculocutaneous perforators cannot be nourished the overlying the entire skin paddle in the musculocutaneous flaps. REFERENCES
Copyright 2007 - European Journal of General Medicine The following images related to this document are available:Photo images[gm07050f2.jpg] [gm07050f1.jpg] |
| |||||||||

{kind=link}
{kind=link}