 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 1, 2008, pp. 9-15 The Association Between Snoring, Daytime Sleepiness And Obesity In Professional Wrestlers Ahmet Ursavaş1, İlker Ercan2, Ramiz Arabacı3, Ufuk Sekir4, Güven Özkaya2, Ezgi Demirdöğen1, Mehmet Karadağ1, R. Oktay Gözü1 Uludağ University, Faculty of Medicine, Departments of Pulmonary Medicine1 and Biostatistics2, and Sports Medicine4, Faculty of Education, Department of Physical Education and Sports3, Bursa, Turkey Code Number: gm08002 ABSTRACT Aim: To investigate the prevalence of snoring, excessive daytime sleepiness and other sleep symptoms in a group of professional wrestlers and to identify the risk factors of snoring in these subjects.
Key words: Snoring, sleepiness, wrestlers INTRODUCTION Snoring is caused by vibration of soft tissues of the upper airway, which in turn is caused by turbulent airflow created by narrowing of one or more cross-sectional areas in the upper airway. Snoring is increasingly recognized as an important public health problem in adults (1). Habitual snoring (snoring on more than 3 nights of week) has been said to be the best predictor of obstructive sleep apnea (OSA) (2). OSA is associated with daytime sleepiness, poor academic performance, stroke, hypertension and ischemic heart disease (3,4).Furthermore, not only habitual snoring combined with OSA or upper airway resistance syndrome, but also habitual snoring alone appears to be linked with impaired daytime functioning in adults (5,6). Population based cohort studies revealed age, obesity, smoking, nasal (eg, septal deviation, rhinitis) and pharyngeal (eg, hypertrophy of tonsils, otitis) problems as independent risk factors for self reported habitual snoring (7,8).Professional wrestlers have some of risk factors for snoring including male gender, high body mass index (BMI) and large neck circumference. On the other hand, sports and physical activity may provide protection from snoring. A low level of physical activity is associated with a higher risk of self-reported habitual snoring (9,10). The aim of this study was to determine the incidence of self-reported snoring, and other sleep symtoms and also to investigate snoring risk factors in professional wrestlers in comparison to age matched men. MATERIAL AND METHODS Study Population This study was performed during a national wrestling tournament. A questionnaire was administered to 55 professional wrestlers and 44 age-matched men. Active sportman in control group were excluded from this study. They were asked to complete the questionnaire on a voluntary basis after informed consent form. Questionnaire The questionnaire was administered by research assistans. All subjects answered nine questions (Have you got insomnia, walking in sleep, talking in sleep, restless legs, snoring, positional snoring, witnessed apnea, day time sleepiness and morning headache ?) about their sleep and snoring habits and self-graded on a scale of 0 to 4, with 0-never, 1-rarely, 2-sometimes, 3- often, and 4-always. Habitual snoring was considered to be the snoring reported as occurring often or always. The questionnaire consisted of Epworth Sleepiness Scale (ESS) for the evaluated excessive day time sleepiness (11). The ESS is composed of eight situations requiring various degrees of vigilance, each with a score from 0 to 3, with a maximum score of 24 and normal score up to 10. The questions are also related to age, height, weight, smoking habits, alcohol intake, general medical history and pharmacological therapy. Neck circumference was measured by research assistants. Statistical Analysis Statistical analysis was performed using the SPSS version 13.0 and Medcalc software. The evaluation of categorical variables was analyzed by using Chi-square and Fisher-exact tests. The statistical significance of differences between the subdivided groups were analyzed with Mann-Whitney U and Kruskal-Wallis tests. The relationship among variables was evaluated by Pearson correlation coefficient. Diagnostic proportions were given along with their 95% confidence intervals (CI). To asses the capability to predict habitual snoring in wrestlers we used the receiver-operating characteristic (ROC) curves, whose circumscribed areas (the area under the curve) gave an estimate of the test’s diagnostic efficiency. P values < 0.05 were considered to indicate statistical significance. RESULTS Clinical characteristics of the wrestlers and control groups are shown in Table 1. Fifty five wrestlers and 44 age matched control subjects completed the questionnaires. Forty (72.7%) of the wrestlers participated at least once to the national wrestling team. Mean age of the wrestlers was 22.0±2.1 years and 22.3±2.2 years of the control subjects. There were 14 (25.5%) smokers among wrestlers and 12 (28.6%) smokers among control subjects. Body mass index (BMI: weight/height2) was 24.7±3.6 kg/m2 in wrestlers and 23.5±2.5 kg/m2 in control subjects. There were no significant differences for age, smoking, alcohol intake and mean BMI between wrestlers and control subjects. Subjects who had BMI higher than 29.9 kg/m2 were accepted as obese. Obesity was significantly more common among wrestlers (14.5%) than in control (2.3%) subjects (p=0.004). Neck circumference was significantly higher in wrestlers (41.1±3.6 cm) when compared to control subjects (36.3±1.9 cm) (p=0.004). Table 1. Clinical characteristics of the wrestlers and control groups
Sleep habits of the wrestlers and the control group are shown in Table 2. Mean total sleep time was reported 8.4±1.2 hour in wrestlers and 6.9±1.1 hour in control subjects. Total sleep time was significantly higher in wrestlers when compared to control subjects (p<0.001). Time to go to sleep before 00.00 o’clock was reported by 38.2% of the wrestlers and 13.6% of the control subjects (p=0.006). Awake time after 08.00 o’clock was reported by 25.4% of the wrestlers and 6.8% of the control subjects (p=0.014). Wrestlers bed time were significantly early and awake time significantly late when compared to control subjects. Table 2. Sleep habits of the wrestlers and control groups
The various degrees of snoring frequencies were distributed as follows: 69.1% never, 16.4% rarely, 5.5% sometimes, 7.3% often, and 1.8% always in wrestlers, and 61.4% never, 18.2% rarely, 13.6% sometimes, 2.3% often, and 4.5% always in control subjects. Habitual snoring rate was reported by 9.1% of the wrestlers and 6.8% of the control subjects. There were no significant differences between wrestlers and control subjects with respect to habitual snoring. Characteristics of habitual and non habitual snorer wrestlers are shown in Table 3. Weight (98.2±29.3 kg in habitual snorer wrestlers, 72.4±14.0 kg in non habitual snorer wrestlers, p=0.046), BMI (29.7±5.5 kg/m2 in habitual snorer wrestlers, 24.2±2.9 kg/m2 in non habitual snorer wrestlers, p=0.026) and neck circumference (45.8±4.8 cm in habitual snorer wrestler, 40.6±3.3 cm in non habitual snorer wrestler p=0.009) were significantly higher in habitual snorer wrestlers as compared to nonhabitual snorer wrestlers. There were no significant differences for mean age and smoking habits between habitual and nonhabitual snorer wrestlers. Table 3. Characteristics of habitual and nonhabitual snorer wrestlers
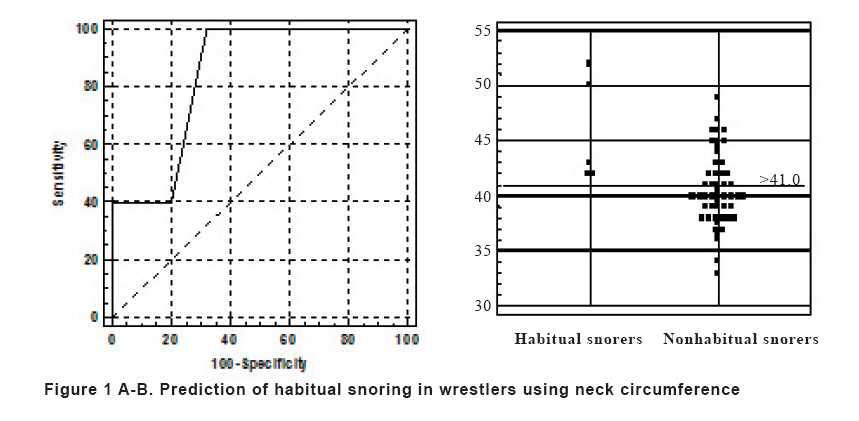
ns: non significant We used ROC analysis to determine the most useful neck circumference in habitual snorer wrestlers. The area under the ROC curve was 0.844 (p=0.012) for neck circumference (Fig 1 A-B). For the neck circumference threshold of 41 cm, predictive sensitivity and specificity for habitual snoring were 100% (95% CI: 48.0% to 100) and 68.0% (95% CI: 53.3% to 80.5%) respectively. Excessive daytime sleepiness, witnessed apnea, and morning headache were reported in wrestlers as 12%, 7.4%, and 36.5%, respectively, and in control subjects as 22.7%, 9.1%, and 51.2%, respectively. The prevalence of these symptoms was not significantly different in wrestlers when compared to control subjects. The mean ESS for the wrestlers was in the normal range and not different from that of the control subjects (5.4±3.7 vs. 4.9±3.7, p=0.342). There were no significant differences for ESS between habitual snorer and non habitual snorer wrestlers (4.7±2.0 vs. 4.9±3.9, p=0.738). ESS greater than 10, which suggests a clinically important degree of daytime sleepiness, was observed in 9.09% of wrestlers and in 13.6% of control subjects. No significant difference was observed in ESS distribution between wrestlers and control subjects. However, obesity was more common among wrestlers than among control subjects. Symptoms of restless leg syndrome (RLS) were reported as often or always in 16.3% of the wrestlers and 4.5% of the control subjects (p=0.105). The various degrees of RLS frequency were distributed as follows: 54.5% never, 18.2% rarely, 10.9% sometimes, 10.9% often, and 5.5% always in wrestlers, and 70.5% never, 15.9% rarely, 9.1% sometimes, 4.5% often, and 0% always in control subjects. Insomnia, sleep talking and sleep walking were reported in wrestlers as 10.9%, 9.1%, and 7.4%, respectively, and in control subjects 11.3%, 2.3%, and 2.3%, respectively (p>0.05). DISCUSSION To our knowledge, this study was the first study, which evaluates the prevalence of sleep disorders in professional wrestlers. The main findings of this study were that there exist no significant differences between wrestlers and control subjects with respect to habitual snoring, daytime sleepiness, ESS, witnessed apnea, morning headache, restless leg, insomnia, sleep talking and sleep walking. We also determined that weights, BMI’s and neck circumferences of habitual snorer wrestlers were significantly higher than that of nonhabitual snorer wrestlers. Population based cohort studies revealed that age, male gender, obesity, smoking, asthma, and nasal congestion are independent risk factors for self-reported snoring (7). Teculescu et al. (12) reported that the prevalence of habitual snoring in middle aged (23-63 years) French males was 32%. They confirmed that age, excess weight, tobacco smoking, blocked nose at night and large soft palate tissue are independently associated with snoring. The prevalence of habitual snoring in 1.910 Asian university student was 25.7%. Male gender showed a trend as an independent predictor for snoring in this study (13). Khoo et al. (14) has shown that snoring was reported by 6.8% of 2298 adults in Singapore. They indicated that male gender, older age, family history, obesity, neck circumference and smoking were independent risk factors for snoring. In our study, we found that habitual snoring rate was reported by 9.1% of the wrestlers and 6.8% of the control subjects. George et al. (15) investigated sleep breathing disorders in professional football players. They estimated the prevalence of sleep breathing disorder to be 14%. Obesity and large neck circumference are major risk factors for habitual snoring and obstructive sleep apnea (OSA). Resta et al. (16) investigated 161 obese subject and 40 age-matched control subjects. They found that neck circumference in men, and BMI in women were strongest predictors of sleep apnea. In another population based study, snoring was reported by 38% of the subjects, and age, BMI and neck circumference were significantly higher in the snorer group. Snoring is generally associated with nasal obstruction and abnormal pharynx exploration (17). In our study, weight, BMI and neck circumference of habitual snorer wrestlers were significantly higher than that of nonhabitual snorer wrestlers. In spite of adjusting age and obesity, a low level of physical activity was associated with higher risk of habitual snoring in obese women and men (9, 18). Previous studies suggested that nasal obstruction is a risk factor for snoring (11, 17). Physical activity has reduced nasal congestion by sympathetic activity (10). However, the clinical importance of this connection is still unknown. Physical inactivity can be a real risk factor for snoring, but it can also be the result of excessive daytime sleepiness. Physical activity can protect from OSA. Moreno et al. (19) investigated the risk of OSA among truck drivers in order to correlate it to potentially related factors, such as serum glucose, cholesterol levels, smoking habits, alcohol and drug consumption and self reported physical activity. They found that the presence of self reported occasional and regular physical activity could be an independent protective factor of OSA. Marchesini et al. (20) analysed 1890 obese patients. They indicated that snoring independently increases the risk of hypertension, whereas physical activity exerts a protection on both snoring and complication. Furthermore, BMI in sportsman is not quite the same as a high BMI in subjects from the general population. The latter individuals are likely to have a much higher percentage of body fat contributing to the high BMI and less lean body mass (muscle) than the sportsman. In our study, we observed that obesity was more frequent among wrestlers and neck circumference was significantly larger in wrestlers than in control subjects. However, the absence of significant differences between the levels of snoring in wrestlers than in control subjects can be associated with the protective effect of physical activity and large muscle mass in wrestlers. Obesity can be associated with excessive daytime sleepiness even in the absence of sleep apnea. Bixler et al. (21) suggest that patients with a complaint of excessive day time sleepiness should be thoroughly assessed for depression and obesity/diabetes independent of whether or not sleep disordered breathing is present. Physical activity has reduced excessive day time sleepiness even with the presence of snoring. Furthermore, sleep complaints can improve sleep quality by initiating some exercise programs (22). Edinger et al. (23) showed that the fit subjects had shorter latencies, lesser wake time after onset, fewer discrete sleep episodes, fewer sleep stage shifts during the initial portion of the night, a higher sleep efficiency and more total slow waves during polisomongraphy than did the sedentary subjects. In our study, the mean ESS for the wrestlers was in the normal range and was not different from that of the control subjects. Despite the fact that obesity is observed more frequently among wrestlers, the absence of difference in daytime sleepiness between wrestlers and control subjects can be explained with high levels of physical activity among wrestlers. Various studies have indicated that daily physical exercise improves the quality and efficiency of sleep in the general population. Alencar et al. (24) analyzed the effect of water exercise weight training and aerobic exercise on total sleep time. They reported that the water exercise group went to bed earlier and the total sleep times were significantly higher in the water exercise group when compared to the other two groups. In accordance with this study, the wrestlers in the present study went to bed earlier and the total sleep time was significantly higher when compared to the control subjects. RLS is a common condition. The prevalence of RLS is estimated to be about 10% and increases with age, smoking, anemia, obesity and renal failure (25). In a recent large scale population based study, a 5% prevalence of weekly symptoms and 2.7% prevalence of at least twice weekly symptoms have been reported (26). In our study, RLS was reported in 16.3% of the wrestlers and in 4.5% of the control subjects. There were no significant differences between two groups. The prevalence of other symptoms in general population has been estimated at approximately 10-15% for chronic insomnia (27), 10-15% for sleep walking, and 5-10% for sleep talking (28). There were no significant differences in the prevalence of insomnia, sleep talking and sleep walking between the general population and the wrestlers in our study. Potential limitations of this study merit consideration. First limitation is that sleep complaints was based on self subjective reports. Second, study population was quite small. In conclusion, although obesity and large neck circumference were quite common among wrestlers, there were no significant differences for habitual snoring, daytime sleepiness, and ESS between wrestlers and control subjects. REFERENCES
Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08002f1.jpg] |
| |||||||||

{kind=link}