 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 1, 2008, pp. 27-35 The Reactive Nature Of Acute Rheumatic Fever: Evidence From Streptococcal Cell Wall Antigen Detection By Immunotechnology Abo-Zenah H1, Al-Hendy A2, Ismail H3 and El-Sayed I3 Menufiya University, Faculty of Medicine & 3Molecular Diagnostic Department, Genetic Engineering and Biotechnology Research Institute, Departments of Internal Medicine1 and Clinical Pathology2, Egypt Code Number: gm08005 ABSTRACT Aim: The life-threatening group A streptococcal (strep) infection and its sequelae, including acute rheumatic fever (ARF), re-emerged as a serious health problem. The fleeting arthritis of ARF is considered a form of reactive arthritis. However, no one has confirmed this by investigating its synovial fluid cells for a possible presence of strep cell wall antigens using western blot in humans. This is the aim of the current study.
Key words: Streptococcal antigen, Rheumatic fever, Rheumatoid arthritis. INTRODUCTION Rheumatic fever (RF) is a catastrophic illness world-wide with an incidence between 10 and 15 million per year (1). In developed countries, world-wide, RF and life-threatening group A streptococcal (strep) infections have re-emerged to become once again a serious health threat (2). A similar situation was noted (3) in emerging nations, including Egypt (4) and the Gulf countries (5). For ARF diagnosis, two major, or one major and two minor manifestations of Johns Criteria accompanied by supporting evidence of antecedent group A strep infection are required. The updated guidelines highlighted a subgroup of “exceptions to Jones Criteria” for patients with chorea, indolent carditis and previous history of rheumatic fever or rheumatic heart disease “RHD” (6). At the present time, echocardiography is insufficient to be the sole criterion for valvulitis in ARF. (7). The term reactive arthritis (ReA) was first used by Ahvonen and co-workers in 1969 (8) to describe joint disease developing after infection elsewhere. Forms of ReA where bacteria have been shown to play a role include pathologic entities in association with Campylobacter (9), Salmonella (10), Chlamydia (11), Shigella (12) infections, Lyme disease (13) and Reiter’s syndrome (14). The pathogenesis ARF-ReA (and arthralgia) is poorly understood (15) although autoimmune mechanisms after group A strep pharyngitis may be involved (16). The arthritogenicity of Strep pyogenes cell wall is attributed to an autoimmune-like disease (17) which for reasons still unclear predominantly manifests itself as ReA (18). The most virulent factor in strep cell wall is surface M protein (19) which immunologically cross-reacts with human tissues (20) including joints (21). An immunogenic factor in M proteins, peptidoglycan (PG), is covalently bound to a group specific polysaccharide (PS) and both (PG-PS) has been implicated in the pathogenesis of animal models of ReA (22). The aim of this prospectively-designed, cross-sectional controlled study is to confirm the reactive nature of acute rheumatic fever in humans by investigating the existence of the streptococcal cell wall antigen, PG-PS, in cells from synovial fluid and peripheral blood by both immunofluorescence and western blotting. MATERIAL AND METHODS Patients This study comprised of two groups of patients; group 1 40 patients with acute rheumatic fever (ARF) and group 2 ten rheumatoid arthritis (RA) patients who served as control group (Table 1). In both groups, the patients were randomly chosen from the patients’ list of the Rheumatology Clinic in the Out-patient Department. Randomization was done manually without the use of a computer algorithm to allocate every other patient on the patients’ list of either disease. The ARF patients have been diagnosed as having initial attack of ARF (15/40) on basis of the updated revised Jones’ Criteria (23) while recurrent attacks depended on history (24) in 25 out of the 40 patients with RF. Apart from the evidenced recent group A strep infection, 22/25 of patients had the classical migratory arthritis (25) while a non-migratory type of polyarthritis that responded within 72 hours to non-steroidal anti-inflammatory drugs was noticed in the remaining 3 patients (26). None of the RF patients with recurrent attacks had an ESR of less than 50 mm in the first hour. Additionally, we observed other minor criteria such as elevated CRP in all and prolonged PR interval on ECG tracing from those with carditis. Of note, 30/40 ARF patients had evidence of RHD. Also, other manifestations such as anemia, precordial chest pains, or epistaxis were variably present. Table 1. Demographic data for the rheumatic fever as well as for the rheumatoid arthritis (control) groups of patients.
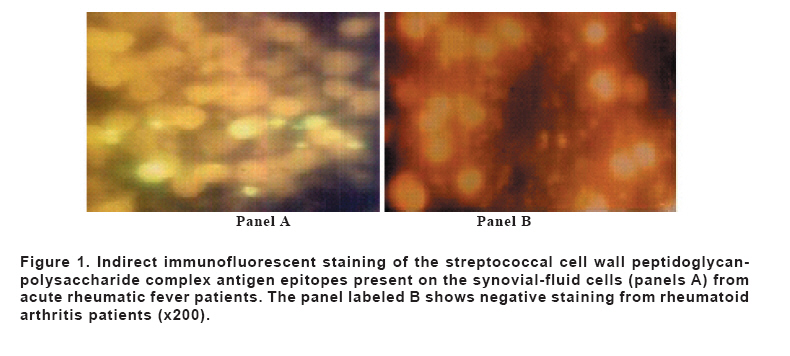
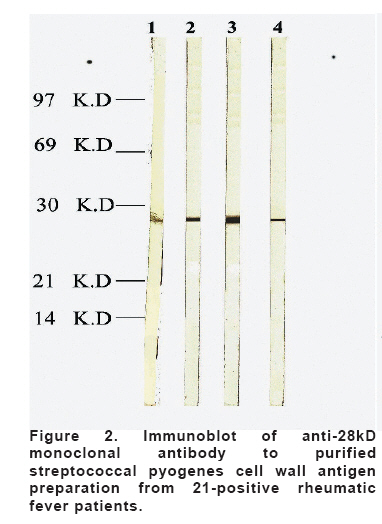
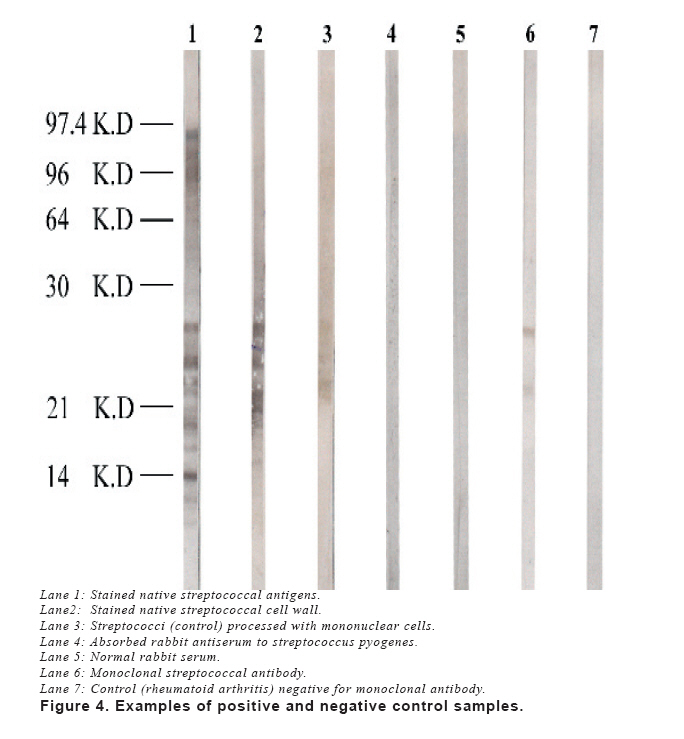
ASO; Antistreptolysin O titer, CRP; C-reactive protein, ns; non significant The only exclusion criterion was the presence of post-streptococcal reactive arthritis (PS-ReA) (27). The controls met the American College of Rheumatology criteria (28) for diagnosing RA and had no history of recent strep infections. The study was approved by the Local Medical Research and Ethics Committee. Informed consent was obtained from all the participants. The study was conducted according to Good Clinical Practice (GCP) guidelines. Specimens Collection Three samples were collected from ARF patients and their RA controls for the planned study; synovial fluids (SF), peripheral blood (PB) (for leukocytes, anti-streptolysin O titer [ASOT] & C-reactive protein [CRP]) and throat swabs. Slow aspiration of SF from knee joint of 32 patients; from elbow in five and from ankle joints of the remaining three patients was done. Part of SF was cultured for viable bacteria while the majority was mixed with heparin (50 IU/ml) in preparation for Ficoll Isopaque gradient centrifugation (at 200g for 10 minutes [min]) to separate mononuclear cells (MNCs). Portion of cell deposit was stored at -70oC and the remaining was suspended in Hank’s balanced salt solution, cyto-centrifuged onto slides at 200 g for 5 min, fixed in ethanol/acetic acid at -20oC, and stored at -70oC to be used for western blotting (WB). At the same time, PB samples were collected and treated by Ficoll–Isopaque gradient centrifugation to separate its MNCs. Bacterial Cultures Blood and SF were cultured in an attempt to isolate the causative micro-organism with special attention to optimize culture conditions for detecting even minute amount of bacteria as reported earlier (10). Sterile swab was taken from the throat and examined for gram-positive microbes and were directly inoculation on blood agar for 24 hrs and extended, if no growth was seen, to 48 hrs. Beta-haemolytic strep were searched for by its characteristic zone of haemolysis, colony morphology, and serology (Patho DX, Latex). Antibodies Used By Immunotechnology Streptococcal cell wall antigen preparation We have prepared strep cell wall fragments from group A strep by using Mickle cell desintigrator as described by Salton and Horne (29). Strep cell wall fragments were then stored at -20oC. Rabbit Polyclonal Antiserum Preparation Antisera against Strep pyogenes were raised by immunization of rabbits with heat-killed bacteria. The rabbits were injected intravenously once a week for 5 weeks with increasing amount of bacteria (0.25, 0.5, 1.0, 1.5, and 2.0 ml of bacterial suspension containing approximately 109 bacteria/ml phosphate-buffered saline [PBS]). The animals were bled 1 week after the final injection. As controls, we used the same antiserum, adsorbed extensively with the immunizing bacteria. Mouse Monoclonal Antibodies We used a commercial mouse monoclonal antibodies specific for PG-PS complex of strep cell wall (ATCC hybridomas 8515[US Pat. 4,596,769]) in this analysis. To ascertain reactivity of antibodies, two controls were used as previously described (30). The first control was the same antibodies used in patients’ specimens and the second one (positive control) was PB-MNCs from a healthy subject that were incubated with the same strep bacteria for one hr and then carefully washed. In-Vitro Indirect Immunofluorescence Rabbit antiserum to strep PG-PS was overlaid to slides and incubated at room temperature (RT) for 30 minutes (min). The slides were then washed with PBS containing 0.2% bovine serum albumin (BSA) and stained with fluorisceinated fragments of antirabbit IgG (1:200) (Sigma Chemicals, St. Louis, USA) at RT for 30 min. Slides were then washed with PBS before being examined with Leitz diaplan-incidence light fluorescence microscope with an Osram HBO 100-W mercury lamp. Other slides were overlaid with mouse monoclonal antibodies specific for strep PG-PS and were then incubated and washed as described before. Lastly, they were stained with fluoresceinated fragments of anti-mouse IgG (1:200) (Sigma Chemicals. St. Louis, USA) before being examined by an investigator who was blinded to the slides code. Electrophoresis and Western blotting (WB) The cell deposits were solubilized in Laemmli’s sample buffer and separated on a vertical sodium dodecyl sulfate-polyacryl-amide slab gel, with a staking gel of 5% acrylamide and a resolving-gradient gel of 5-17.5 %, or 10-12.5 % acrylamide. Standards of known molecular weight were included in each gel run (electrophoresis Low Molecular Weight Calibration Kit, Pharmacia Fine Chemicals AB, Uppsala, Sweden) (31). For WB, the separated components in the gel were immediately transferred electrophoretically onto nitrocellulose sheets (HAHY 00100; pore size, 0.45 µm/Miilipore; SA, France) with the use of a Transphore apparatus (LKB-Bromma, Sweden) and pre-chilled TRIS-glycin buffer (pH 8.3) for 1.5 hrs. Molecular weight standards were visualized with amido-black staining. Non-specific binding sites of nitrocellulose were blocked by overnight incubation at 4oC in PBS (pH 7.4) containing 10% horse serum. After 5 washes with PBS, nitrocellulose sheets were cut into strips and each was stained separately and was allowed to react overnight at 4oC with a 1:300 dilution of rabbit antiserum or with a 1:20 dilution of mouse monoclonal antibody in PBS with 10% horse serum. They were then rewashed and incubated for three hrs at RT with horseradish-peroxidase-labeled anti-rabbit or un-conjugated rabbit anti-mouse immunoglobulins (DAKO Immunoglobulins, Copenhagen, Denmark). The mouse blots were again washed and incubated with horseradish-peroxidase-labeled anti-rabbit immunoglobulins. After three washes, the strips were developed with 4-chloro-1-naphthol (Sigma Chemicals, UK) (32). Statistical analysis Variables are expressed as mean±SD, unless otherwise stated. The chi-squared test, student t-test and Mann-Whitney test were used as appropriate. The correlation coefficient was estimated between qualitative variables by Spearman’s test. The statistical significance was established at a p value of ≤ 0.05. Non-significant level was noted as NS. The statistical analysis was performed using the Social Package for Statistical Science (SPSS) version 10. RESULTS The ARF patients were significantly younger (t-test p<0.0001) with lesser number of joints affected by arthritis compared to RA control group (3+1 vs 11+5). Likewise, the level of anti-streptolysin O titer (ASOT) in ARF was significantly higher (t-test, p<0.001) than the corresponding figure in RA patients. However, the difference in C-reactive protein (CRP) level was non-significant (NS) between the two groups (table 1). Of note, extensive bacterial cultures of SF, blood and throat were negative for serological evidence for microbial infection with any of the organisms known to cause ReA, particularly salmonella, chlamydia, shigella, or brucella. Immonofluorescence (IF) By in-vitro IF, fifteen out of our forty ARF patients (37.5%) showed strep PG-PS antigens with rabbit polyclonal antiserum as well as with mouse monoclonal antibodies in their SF- and PB-Cs. The proportion of positive results within ARF group was statistically significant (Chi-square=3.72, p=0.048) and is significantly higher than the negative IF observed in RA (Mann-Whiney p= 0.022). The observed positive staining was identical with both antibodies and was seen mostly in polymorphnuclear- and to a much lesser extent in mononuclear-cells (Figure 1, A). On the average, five to ten percent of the cells seen in the examined slides showed granular staining of cytoplasm. Negative staining was noted in samples from all RA control group (Figure 1, B). Western Blotting Both, SF- and PB-cells from 21 out of the investigated 40 patients (52.5%) with ARF were positive on WB analysis using monoclonal antibodies specific for strep PG-PS antigen. Within this group, the proportion of positive results was statistically significant (Chi-square=8.2, p=0.0008) and a significant difference between WB observed in ARF patients and the negative results seen in all RA patients was noticed (Mann-Whitney; p=0.003). The observed bands were of the same molecular weight but with varying intensities. A light band with a molecular weight of 28 kD was visualized in SF-Cs of fifteen patients who have recent ARF (Figure 2, lane 1) and a sharper band with the same molecular weight was seen in PB-MNCs of some of them (Figure 2, lane 2). In the remaining patients who had repeated attacks of ARF polyarthritis, a strong band with a molecular weight of 28 kD was visualized in SF-Cs slides (Figure 2, lane 3) as well as in PB-MNCs (Figure 2, lane 4). Samples from 27 (67.5%) patients with ARF were positive in slides of both SF-Cs and PB-MNCs with rabbit polyclonal antiserum and this proportion was significant (Chi-square=4.9, p= 0.027). Similar to our observation with monoclonal blots, the noted reactivity on using the polyclonal antiserum in ARF was much higher than the non-reactive pattern of blots in controls and the difference was statistically significant (Mann-Whitney; p= 0.0001). Interestingly, patients with arthritis only showed a band with a molecular weight of 26-29kD (Figure 3, lane 2) in their SF-Cs and PB-MNCs (Figure 3, lane 3). However, the reactivity pattern was much broader in those having arthritis in addition to carditis, (Figure 3, lane 4). Of note, Lane 1 of the same figure showed a control normal rabbit serum. In addition, we observed a significant correlation between the positive reactivity with the application of mouse monoclonal antibodies and that with rabbit polyclonal antiserum (r=0.729, p=0.0001). We, however, failed to detect any significant correlation between the positive reactivity with either antibody and the elevated ASOT or CRP in ARF patients. Figure 4 displayed examples of positive and negative staining of SF-C from patients with ARF. The reactivity of rabbit antiserum and monoclonal antibodies against strep pyogenes and against PB-MNCs incubated with the bacteria in vitro for one hour are also shown. With both antibodies the reactivity pattern of ingested bacteria was considerably narrower than that of native bacteria. DISCUSSION In this study we detected streptococcal (strep) antigens in synovial-fluid (SF) and peripheral-blood mononuclear cells (PB-MNCs) from patients with acute rheumatic fever (ARF) with the use of immunotechnology including both indirect immunofluorescence (IF) and western blot (WB) analysis. Despite a century of research, the pathogenesis of rheumatic fever (RF) remains incompletely understood (33, 34). One of the major obstacles to understanding the pathogenesis of RF is the inability to establish an animal model of rheumatic heart disease. However, the cytotoxicity (enzyme-induced) theory and the immunologic (immune-mediated) theory have been proposed for such explanation. Genetic susceptibility (host factors) is present in 3-5% of people and the mode of inheritance is however, uncertain; autosomal recessive or autosomal dominance with partial penetrance has been suggested. The basis for this genetic susceptibility is again not known despite the observed association with HLA class II alleles (D8/17) (35). Although still obscure, the pathogenesis of ARF requires primary infection (organism factor) of the throat by certain serotypes of group A strep (the concept of Rheumatogenicity). M serotypes 1, 3, 5, 6, 14, 18, 19, 24, 27 and 29 are the most frequently implicated. The pathogenic factor (s) are not known although M protein, the hyaluronic acid capsule, the cell wall-associated group-specific carbohydrate, and the cell membrane have all been suggested (36). Likewise, the secreted GAS erythrogenic toxins (37). Group A strep also has components which act as superantigens that selectively stimulates T-lymphocytes without the need for antigen presentation. By IF, we were able to see strep cell wall antigen epitopes in 37.5% of the examined ARF samples. The pattern of staining was similar to that reported by previous investigators being entirely cytoplasmic and variable in its physical form from fine to large granular. However, we failed to see any of the vacuolar forms observed by them (30). The presence of positivity was low as IF can detect epitopes of interest only when present on cell side that is exposed to staining. No strep antigens were observed in any of examined material from RA patients with this technique. In this study, we did not use in-vivo IF because of the well-described label dissociation from relevant bacterial structure by in-vivo degradation (38). By WB analysis, we have been successful in detecting strep antigens after application of rabbit polyclonal anti-serum, in 27 out of 40 ARF patients (67.5%). The proportion of positive staining was substantial and its band was wide and of molecular weight (MW) ranging from 26-29 kD while the remaining 13 patients showed multiple bands varying in their MW from 55-58 kD. Further, we observed these antigens in 21 (52.5%) of ARF patients after using mouse monoclonal antibodies to peptidoglycan (PG)-polysaccharide (PS) complex of strep cell wall. The positive bands have a MW of 28 kD. None of used antibodies detected positive result on control samples from patients with RA. The percentage of positive results was higher on using WB technique compared to indirect IF since it detects digested cell wall components rather than cell wall antigen epitopes. The positive results of monoclonal antibody immunoblot were considerably higher than negative results. The presence of PG component of the strep PS as a potential key player in the development of ARF was confirmed because we used monoclonal antibodies as well. However, other bacterial degradation product can not be excluded. A significant association was detected between the results of immunoblotting analyses by using polyclonal antibodies and monoclonal antibodies inferring shared epitopes by the antigens To the best of our knowledge, there is not yet established similar research done on Egyptians with ARF using both IF and WB for cell from both peripheral blood and synovial fluid. However, other investigators have reported more or less similar data on studying ReA following other infections with salmonella (10), Yersinia enterocolitica infection (39), Reiter’s Syndrome (40) and Lyme disease (13) in patients with different genetic backgrounds. Our result with WB also indicates extensive processing of strep cell wall as we observed a broader band with subsequent granular staining of cytoplasm. This is similar to the literature reported in Yersinia-triggered ReA (30). Further, the finding of strep cell wall PG-PG after a latent period following infection was not surprising as it is relatively resistant to digestion (14) and such inhibition of effective bacterial clearance may be mediated by antigen-specific interleukin-10 secretion (41). We failed to find any correlation between ASOT and strep PG-PS antigens detected by using either IF staining or WB immuno-reactivity. This is in concordance with the findings of Heymer and associates (1976) (42). Likewise, and similar to what has been reported by Johnson and co-workers (1984) (43), we failed to observe any significant association between CRP and these antigens. Such findings exclude any possible use for either as surrogate marker of ARF. In conclusion, the reactive nature of acute rheumatic fever in humans may be considered due to our observation of microbial (streptococcal) antigens in affected joints and in peripheral blood along with absence of viable bacteria. Also, detection of these streptococcal antigens is common and would be easier with the immunotechnology. Acknowledgment The Authors are grateful to Prof. Farouk Fouad, Menufiya University School of Medicine who helped in preparation of this manuscript. Also, we are expressing our sincere appreciation to the invaluable help of DR. Emma Davis who improved a lot the fluency of English Language of this article. REFERENCES
Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08005f3.jpg] [gm08005f4.jpg] [gm08005f2.jpg] [gm08005f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}