 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
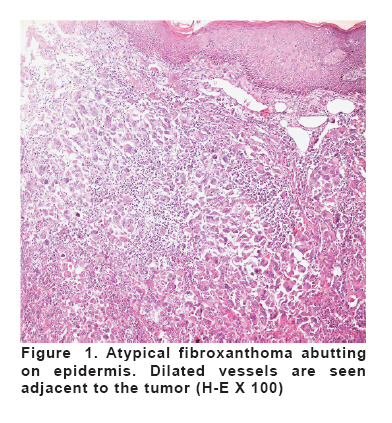
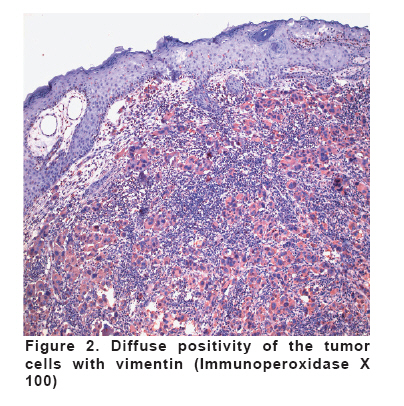
European Journal of General Medicine, Vol. 5, No. 1, 2008, pp. 45-47 Atypical Fibroxanthoma Of The Eyelid Adil Kılıç1, Mustafa Kösem2, Adnan Çınal1, Tekin Yaşar1, Ahmet Demirok1 Yüzüncü Yıl University, Faculty of Medicine, Departments of Ophthalmology1 and Pathology2, Van, Turkey Code Number: gm08008 ABSTRACT Atypical fibroxanthoma (AFX) is probably a neoplasm of fibrohistiocytic lineage. The tumor arise in the skin and has strikingly atypical properties. We report a case of AFX that was excised from the left lower eyelid of a twelve-year-old girl. The nodular mass was reported as AFX. Though this tumor has the capability to recur aggresively, no recurrence was noted in the present case. Malignant fibrous histiocytoma, atypical fibrous histiocytoma, squamous cell carcinoma, sarcoma, dermatofibroma protuberans, and reticulohistiocytoma should be included in differential diagnosis. Key words: Atypical fibroxanthoma, eyelid, INTRODUCTION Atypical fibroxanthoma (AFX) is an uncommon, fibrohistiocytic tumor of the skin that occurs due to actinic damage in the elderly (1). AFX rarely affects eyelid (2). It appears as solitary nodule that smaller than 2 cm (3). Boynton was the first to describe a case of AFX involving the eyelid in the literature (2). Aggresive recurrence was reported in few AFX cases, despite the benign nature of the tumor (4). Surgical excision with tumor-free borders is curative (1). Malignant fibrous histiocytoma, atypical fibrous histiocytoma, squamous cell carcinoma, sarcoma, dermatofibroma protuberans, and reticulohistiocytoma should be included in differential diagnosis (1,5,6). As far as we are aware, the present case of AFX is the third one involving the eyelid in the ophthalmic literature (1,2). CASE A twelve-year-old girl presented with a nodular mass involving the left lower eyelid. The mass increased in size over several months. The slit-lamp examination of the left eye revealed an encapsulated pinkish-white, elastic, exophitic mass that was measured 10 × 8 × 5 mm. An excisional biopsy was performed at our eye clinic. On examination the visual acuity was 20/20 in either eye. Both the slit-lamp examination of the right eye, and the fundus examination of either eye revealed normal findings. No proptozis was observed. Excursions were full. The remainder of her ophthalmological examination was not remarkable. No recurrence was noted five months after excision. The pathologic findings were consistent with AFX. Macroscopically, the tumor mass was encapsulated with its off-white and solid cut surface. Microscopically, the tumor tissue was characterized by bizarre cells arranged in a haphazard pattern. The tumor was covered by squamous epithelium. There were dilated capillaries and lymphatics adjacent to the tumor (Figure 1). No necrosis was noted. The tumor cells were round-shaped and exhibited multinucleation, pleomorphism and numerous mitotic figures. Inflammatory cells intermingling with the tumor cells were detected. Immunohistochemically, the tumor cells showed strong and diffuse positivity with vimentin (Figure 2), widespread positivity with CD68, and diffuse, but weak positivity with CD99. DISCUSSION In 1973, AFX of the skin was recognized as a tumor that behaves in a benign fashion, despite its atypical appearance (7,8). Later on, its metastatic potential was described in 1986 (8). Associations with metastases and poor prognosis include recurrence, previous radiation, deep invasion, vascular invasion, and tumor necrosis (2). AFX has male dominancy (9). AFX is a member of the family of spindle-cell and pleomorphic neoplasms of skin (6). AFX is reactive for cathepsin-B, alpha-1-antichimotrypsin, and alpha-1-antitrypsin (6). Furthermore, AFX stains positively for vimentin, and negatively for S100 and epithelial membrane antigen (1). AFX was also reported to be positive for CD68 and CD99 (10,11). The tumor cells in our case showed strong and diffuse positivity with vimentin, widespread positivity with CD68, and diffuse, but weak positivity with CD99. AFX has substantial morphologic and immunohistochemical similarities to malignant fibrous histiocytoma (MFH) (6). MFH stains positively for vimentin (12). MFH occurs in deep soft tissues and requires complete excision with wide margins. On the contrary, AFX originates in the dermis and localized excision is adequate for the treatment (1). AFX is superficially located with epidermal ulceration or atrophy of the overlying skin (1). AFX has a predilection for head and neck, whereas MFH commonly involves lower and upper exremities (13). It is also difficult to differentiate the neoplasm from squamous cell carcinoma (SCC) (1). SCC stains positively for cytokeratin and epithelial membrane antigen, but does not stain for vimentin and S100 (1). Solar radiation is a definite risk factor for AFX, whereas irradiation is a probable risk factor for the tumor (3). Our case denied any irradiation. Despite the 7-12% recurrence rate reported in the literature, our case did not recur five months after excision (3). To conclude, diagnosing AFX of great importance for the ophthalmologists, since the tumor can either invade the orbit locally or probably metastatise, and earlier localized excision of the tumor by histologic examination of its surgical borders, solely, controls the the disease. REFERENCES
Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08008f1.jpg] [gm08008f2.jpg] |
| |||||||||

{kind=link}
{kind=link}