 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
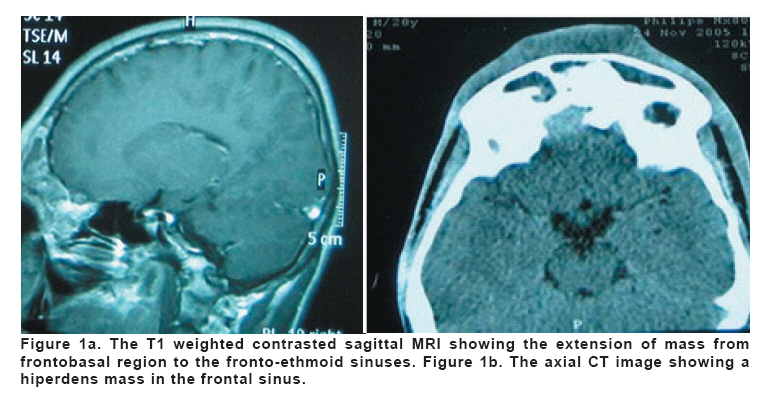
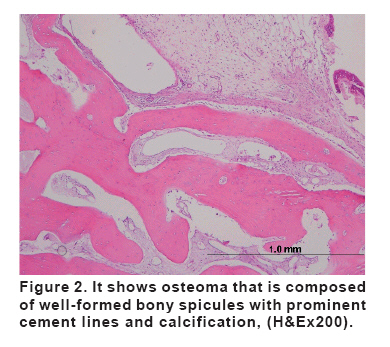
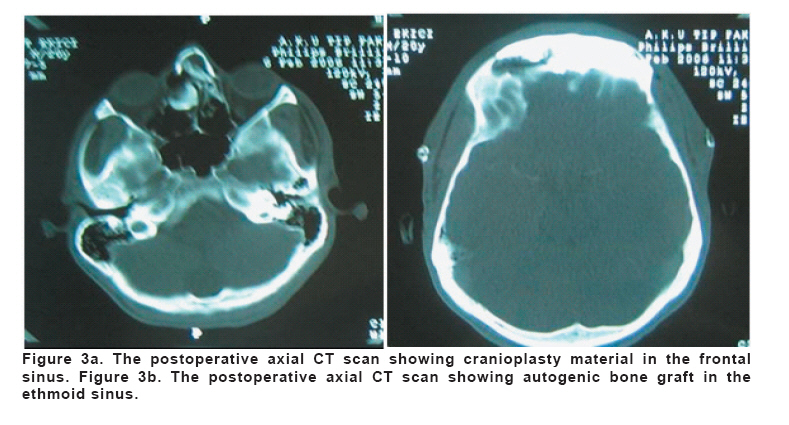
European Journal of General Medicine, Vol. 5, No. 1, 2008, pp. 48-50 Ethmoid Osteoma With Frontal And Frontobasal Extension Murat Coşar1, Olcay Eser1, Adem Aslan1, Abdullah Ayçiçek2, Sefa Dereköy2, Hüsniye Dilek3 Kocatepe University, Faculty of Medicine, Departments of Neurosurgery1, Otorhinolaryngology2 and Pathology2, Afyonkarahisar, Turkey Code Number: gm08009 ABSTRACT Paranasal sinus osteomas are benign slow growing tumors, occasionally known to cause complications for a long time. Frontobasal extension of paranasal sinus osteoma is an uncommon localization. We present a 20 year-old-man admitted to our clinic with a complaint of pus drainage and wound from forehead for 2 weeks. The radiological images of the patient revealed a mass mimicking osteoma and extending into the frontal sinus and frontobasal area with a chronic infection. The patient was initiated antibiotics for 2 weeks and the mass was extirped through the destructed anterior wall of frontal sinus. The histopathological diagnosis was osteoma and the patient was discharged uneventfully at the 7th day after the operation. Key words: Frontal, ethmoid sinuses, osteoma, surgical treatment INTRODUCTION Although the frontobasal extension of the osteoma is uncommon, it is the most frequent benign tumor of the paranasal sinuses (1-5). It is a slow growing, osteogenic neoplasm that usually originates from the frontal and ethmoid sinus and much less frequently seen in the maxillary and sphenoid sinuses (1). The tumor is generally asymptomatic with incidental radiologic findings but, complications of paranasal sinus osteomas have been known for a long time (6,7). Pain, sinus obstruction and infection are initial symptoms of growing osteomas in ethmoid sinus. Facial deformity, visual changes, or intracranial complications may occur when the lesion become large (1,4,8,9). In this report, we present an ethmoidal osteoma extending into the frontal sinus and frontobasal which was treated surgically. CASE A 20 year-old-man admitted to our clinic with a complaint of pus drainage and wound from forehead for 2 weeks. The history of the patient revealed skin blushing and swelling in the forehead for 2 months and progressive frontal headache for one year which had become more intense for 6 months. The physical examination of the patient revealed fore head infection under the skin. The neurological examination of the patient was normal. Anterior wall destruction of frontal sinus was detected in the direct plain radiographies. Cranial computerized tomography (CT) and magnetic resonance imaging (MRI) showed that the mass was arising from posterior ethmoid cells, extending posteriorly to frontobasal region and frontal sinus, and destructing the anterior wall of frontal sinus. Additionally, infection was accompanying to the mass in the frontal sinus (Figure 1a, b). Surgical removal of the lesion was planned and forehead pus and infected materials extending to the frontal sinus were drained with a needle punction and antibiotics (Ceftriaxon 2x1 gr) was initiated for 2 weeks. The skin blushing and swelling became normal after 2 weeks and operation was planned. Bifrontal skin incision was performed to the patient. The frontal sinus, posterior ethmoid cell and frontobazal located mass was extirped through the destructed anterior wall of frontal sinus. Authogenic grafts from frontal bone were mounted between the frontal and ethmoid sinus. Additionally, lipoid tissues transferred from abdominal region located to the bottom of the frontal sinus and cranioplasty was performed to the roof of frontal sinus. The histopathological examination revealed the osteoma that composed of well-formed bony spicules with prominent cement lines and calcification.They may demonstrate osteoblasts, osteoclasts, and osteocytes and occasionally may even demonstrate bone marrow elements (Figure 2). The course was uneventful and the patients was discharged at the 7th day after the operation. The neurological and physical examination and follow-up cranial CT scans were normal which were performed 1 month and 6 months after the operation (Figure 3a, b). DISCUSSION In relation to its dimensions and localization, a sinonasal osteoma can give rise to functional symptoms, infection, ophtalmologic and cerebral complications etc (1,10,11). Most authors agree that symptomatic osteomas should be treated surgically, but there is some controversy regarding the management of asymptomatic osteomas (5,12,13). According to Savic and Djeric (3), asymptomatic osteomas should be operated upon if they extend beyond the frontal sinus boundaries, if they can be demonstrated to be enlarging on repeated radiological examinations, or if they are located near the frontonasal duct. Chronic infection of frontal sinus due to its obstruction had caused to the destructed anterior wall of frontal sinus and severe headache. Although the first surgical removal of an osteoma of the paranasal sinuses was performed and recorded as early as 18 th century, type of surgical approach of these tumors have not yet been established (3). Osteoplastic flap operation, Reidel’s operation, and lateral rhinotomy are the main open procedures which have been used for many years. Osteoblastic flap technique should be used for the frontal and ethmoid sinuses osteomas. Reidel’s operation may be chosen when the osteoma has destroyed the anterior wall of the frontal sinus, and in extremely large osteomas penetrating into the anterior cranial fossa. Additionally, lateral rhinotomy should be used for very large osteomas affecting the frontal, ethmoid and maxillary sinuses (3). The recent development techniques has offered endoscopic approach for solitary ethmoidal osteomas (1). Due to destructed anterior wall and frontobazal extension of our case we decided to perform a modified Reidel’s operation. We planned osteoplastic approach but, because of the anterior wall destruction of frontal sinus we could not perform. So, we performed a modified osteoplastic approach. Direct plain radiographies may show the destruction of bones, additionally may help to plan the operation. CT is gold standard for diagnosis and follow up of these kind of lesions. MRI may help for diagnosis of pus and soft tissue included osteomas as seen in our case. As a conclusion, we think that the silent osteomas of the paranasal sinuses must be followed carefully. It may obstruct frontal sinus and may trigger infection. REFERENCES
Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08009f2.jpg] [gm08009f3.jpg] [gm08009f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}