 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 2, 2008, pp. 84-89 Conjunctival Z-plasty For Pterygium: Comparison With Conjunctival Autografting Murat Özdemir Sütçü İmam University, Faculty of Medicine, Ophthalmology Department,
Kahramanmaras, Turkey Code Number: gm08016 Aim: High recurrence rate is the most common problem after the pterygium excision surgery, and the adjunctive therapies performed to reduce the recurrence rate have severe complications. The aim of this study was to compare the safety and efficacy of conjunctival Z-plasty and conjunctival autograft application in primary pterygium surgery.
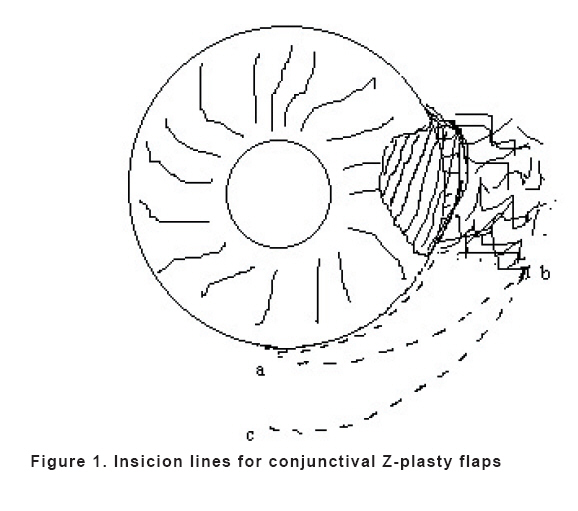
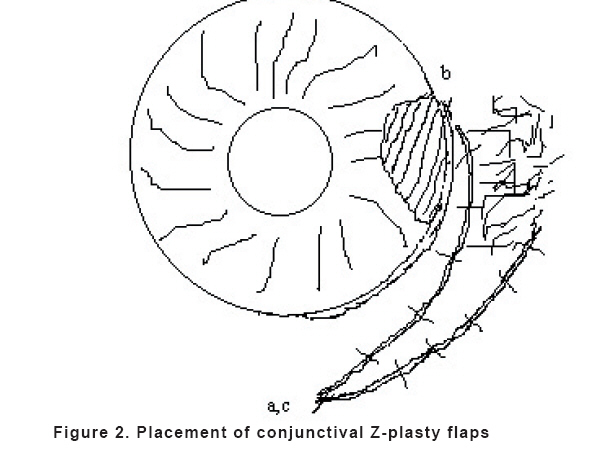
Key words: Primary pterygium, surgery, conjunctival autografting, conjunctival Z-plasty, recurrence INTRODUCTION Pterygium is an abnormal overgrowth of the conjunctiva onto the cornea. Surgical management is the choice of treatment when persistent discomfort, visual distortion, and restricted ocular motility bothers patient’s life.1 Although an easy procedure, the main problem with the surgical excision of the pterygium is the recurrence rate, which can be as high as 30 to 82% (1-3). Recurrence is usually defined as the growth of fibrovascular tissue across the limbus onto the cornea in the area of previous pterygium excision. To reduce the recurrence rate, adjunctive therapy such as mitomycin-C, 5-fluorourasil, beta-irradiation, and thio-thepa have been used after the pterygium excision with varying success (4-8). Although all of the adjunctive therapies mentioned above achieved a significantly greater reduction in the recurrence rate than surgery did alone, mitomycin-C application was reported as the most effective procedure (4). However, the complications of the adjunctive therapies including severe and prolonged ocular hyperemia, allergic reactions, punctate keratopathy, corneal melting, scleromalacia, scleral necrosis, corneal perforation, cataract and secondary glaucoma have been revealed (9-13). To avoid such complications, specific surgical techniques such as conjunctival autografting, amniotic membrane transplantation, conjunctival rotation flaps, and conjunctival Z-plasty have been used in the pterygium surgery (14-17). Conjunctival autografting is a safe and an effective procedure to reduce the recurrence of pterygium (18). This method, however, is not free of complications, and technical difficulties it possesses prevent it from being the method of choice (19-20). To the best of our knowledge, conjunctival Z-plasty without adjunctive therapy has been previously studied by Wilson and Bourne (17). However, the authors have not mentioned about the recurrence rate or other complications in their report. In this study, we compared the safety and efficacy of conjunctival autografting with conjunctival Z-plasty in primary pterygium surgery without employing any adjunctive drug. MATERIAL AND METHODS This study included 42 eyes of 42 consecutive patients matched eligibility criteria and underwent excision of the primary pterygium in our clinic. All patients gave informed consent and the study protocol followed the guidelines of the Declaration of Helsinki. Our indications for surgery were cosmetic disfiguration, visual distortion, and persistent ocular discomfort. The inclusion criteria were an age greater than 20 years, primary progressive pterygium (fleshy, vascularized, and encroached more than 2 mm onto the cornea), no other ocular surface pathology, no systemic pathology, follow up of at least 6 months, and nasal localization. Atrophic or recurrent pterygium, collagen vascular disease, an age greater than 60 years, ocular surface disorder, dry eye, history of any ocular surgery or trauma were accepted as exclusion criteria. All patients underwent complete ocular examination before surgery. Only right eye of the patients who were operated bilaterally were included in the study for the statistical reliability. Patients were randomly divided into two groups. Twenty-one patients were treated by conjunctival autografting technique (autograft group), and the other group of 21 patients was treated by conjunctival Z-plasty (Z-plasty group). Operation time was recorded for each patient. It was measured from excision of pterygium head to the end of the surgery. Operations were performed under topical anaesthesia that consisted of one drop oxibuprocaine 0.4% application, and intraconjunctival anaesthesia that consisted of 0.5 cc lidocaine 2% injection. The pterygium was avulsed from the apex and then peeled and excised by the help of a Westcott scissors. Minimal cauterization was performed to obtain hemostasis. The conjunctival autografting in the autograft group was performed using the technique developed by Kenyon. The technique consisted of transferring of free conjunctival graft from the donor site in the superotemporal bulbar quadrant of the conjunctiva to cover the bare sclera in the excised pterygium area (14). In the Z-plasty group, the technique developed by Wilson and Bourne was used with a little modification (Figure 1, 2) (17). Intact conjunctival tissue was dissected from limbus until six-hour quadrant (Figure 1a). Than, the discission was directed towards the base of the pterygium (Figure 1b). After that, an intact triangular flap was produced cutting the conjunctiva towards the inferior fornix (Figure 1c). The end of the intact flap was sutured the superior limbal conjunctival edge of the bare sclera arising from pterygium excision (Figure 2b). The end of the other triangular flap including remaining pterygium tissue was anchored the top of the bed of the intact triangular flap (Figure 2a,c). Than, the edges of the flaps were sutured each another. All suturations were performed with 8/0 vicryl suture material. All eyes received postoperative treatment of 0.1% dexamethasone sodium and 0.3% tobramycin 4 times a day for 4 weeks. All patients were evaluated on the first, seventh, and fifteenth postoperative day, in each month in the first six months, and in each 3 months thereafter. Follow up period ranged from 7 to 28 months (mean 18 months) in the autograft group, and 8 to 26 months (mean 17 months) in the Z-plasty group (p>0.05). At each visit, patients were evaluated for visual acuity, the presence of recurrence, injection, graft edema, wound healing, dellen, loose graft, and symblepharon. Recurrence was defined as the postoperative growth of 2 mm fibrovascular tissue onto the cornea and was confirmed by two surgeons. The statistical analyses were performed with Mann-Whitney U test for mean ages and operation time, and with chi-square test for sex and incidence of recurrence and complications. A p value of less than 0.05 was considered statistically significant. RESULTS There was no significant difference between the two groups for demographic characteristics (p>0.05) (Table 1). Table 1. Demographic characteristics of the study patients
Recurrence (4.7%) was observed in one patient in the autograft group at the 3rd postoperative month. One (4.7%) recurrence occurred in the Z-plasty group. In the autograft group, graft edema was observed in two (9.5%) eyes, loose graft in one (4.7%) eye, and tenon’s granuloma in one (4.7%) eye. Medical therapy was adequate to manage these complications. A sauture loosening which did not require revision was observed in one (4.7%) eye in the Z-plasty group. Moreover, recurrent pterygium was observed in one (4.7%) patient at 4th month. No significant difference was observed between the groups in recurrence and complication rates (p>0.05). Mean operation time was significantly shorter in the Z-plasty group (16.10 ± 2.0 (range, 13-20) minutes than that in the autograft group [36.14±3.8 (range, 30-45) minutes (p<0.001)]. DISCUSSION Simple excision of pterygium has a high recurrence rate (30-82%) (1-3). To avoid recurrence, various medical and surgical methods are employed. The ideal treatment method of pterygium should both prevent the recurrence and have no adverse effect. The ideal procedure owning these advantages has not been developed yet. Mitomycin-C application and conjunctival autografting are the two most commonly used adjunctive treatment methods in pterygium surgery (18). Employing postoperative mitomycin-C drops or intraoperative single dose mitomycin-C was reported to reduce the recurrence rate after pterygium excision as low as 0% to 12% (5,21,24). Anduze, in a ten-year study, reported mild and easily resolved adverse effects with the single intraoperative application of 0.1 cc of 0.4 mg/ml of mitomycin-C into the subconjunctival space (4). However, the serious sight-threatening complications of mitomycin have been reported even if it was used in a minimum concentration and for a minimum period (13,24,25). These reports raised questions regarding the safety of mitomycin-C in pterygium surgery. Recently, the conjunctival autografting is used successfully in pterygium surgery to prevent the recurrence. The most report revealed that this procedure had a recurrence rate of 0% to 7% (3,14,18). Stark et al suggested that conjunctival autografting is the best option in the treatment of advanced primary and recurrent pterygium (26). However, Lawallen and Chen et al reported a 21% and 39% recurrence rate after conjunctival autografting (28,29). Moreover, it may cause many problems such as graft edema, graft necrosis, subconjunctival hematoma, granuloma of the tenon, corneoscleral dellen, epithelial inclusion cysts, and donor site fibrosis, and there can be donor graft handling (9,14,27,28). In addition, conjunctival autografting has other complications including a technical difficulty with extended operation time and expense, and patients discomfort originating from multiple suture knots. More recently, conjunctival rotation autografting, as an alternative to conjunctival autografting, has been suggested in pterygium surgery (15,19). Jap et al revealed a 4% recurrence rate and they didn’t report any significant complication (15). But, these authors suggest this procedures in only cases in which it is not possible or not desirable to use the superior conjunctiva as a donor source. And also, this procedure can not be used in cases with large bare scleral area. Conjunctival Z-plasty was firstly defined by Wilson and Bourne, who did not report any recurrence or significant complication (17). In our study the recurrence rate was 0% in the Z-plasty group, and it was similar to the recurrence rate in Wilson and Bourne’s study (17). We did not observe significant complication in the Z-plasty group. Conversely, the recurrence rate was 4.7% in the autograft group, which corresponds to the most reports and more, mild complications were seen in four (19%) eyes. Operation time is very important regarding to comfort of patient and surgeon in the surgery. Recently, several new studies are performed to shorten the operation time of the most surgical procedures. In our study, operation time was found shorter in the Z-plasty group than in the autograft group. Wilson and Bourne did not investigated the operation time of this procedure (17). We believe that the placement of healthy conjunctiva between the pterygium tissue and cornea functions as a barrier and prevents the overgrowth of pterygium tissue onto the cornea in the conjunctival Z-plasty technique (14,30). Changing the direction of pterygium may also be play a role in reducing the recurrence rate in this procedure. In conclusion, conjunctival Z-plasty and conjunctival autografting appear to be equally safe and effective in reducing the recurrence rate following primary pterygium surgery. Conjunctival Z-plasty can be useful and reliable alternative procedure for pterygium surgery to reduce the recurrence after primary pterygium excision. In our results, conjunctival Z-plasty is more advantageous than conjunctival autografting because of its shorter operation time and easier application. REFERENCES
Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08016f1.jpg] [gm08016f2.jpg] |
| |||||||||

{kind=link}
{kind=link}