 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 2, 2008, pp. 90-94 Vesicoureteral Reflux Incidence In Siblings Of Children With Reflux: Is Screening Required? Fatma Dursun1, Muferet Erguven1, Yasemin User Denizmen1, Memduh Dursun2, Sabri Yılmaz2, Mehtap Haktanır Abul1 Goztepe Training and Research Hospital, 1Department of Pediatrics, Istanbul University, Istanbul Faculty of Medicine, 2Department of Radiology, Istanbul, Turkey Turkey. Code Number: gm08017 Aim: The purpose of this study was to evaluate prospectively the age-related incidence and severity of primary vesicoureteral reflux (VUR) in siblings of children with reflux and to conclude whether screening of this group is required or not.
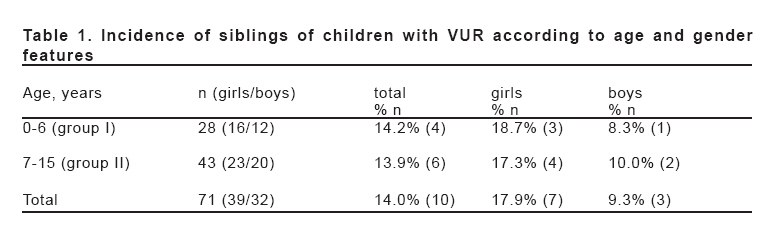
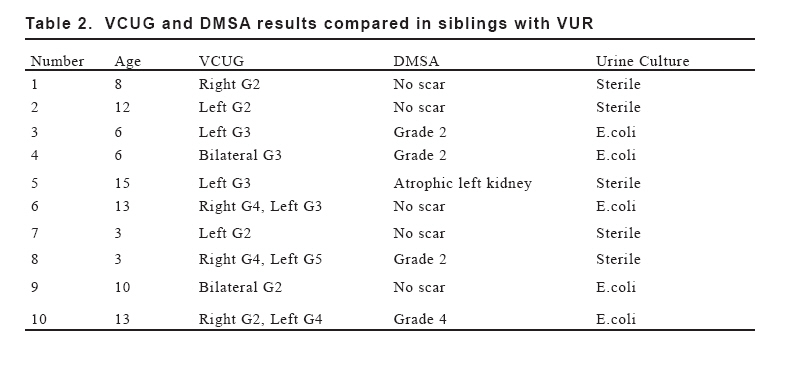
Key words: Primary vesicoureteral reflux, siblings of children with reflux, screening INTRODUCTION Primary vesicoureteral reflux (VUR) is the most common anomaly in children with urinary tract infections (UTI). It is found in 26-59% of children with this disease. Reflux nephropathy, which reflects the damage of renal parenchyma, is the most severe complication of VUR. Early diagnosis and adequate treatment of VUR is supposed to prevent nephropathy. It is estimated that reflux nephropathy is responsible for 5-15% of renal failure cases in adults, and it is also one of the most frequent causes of severe hypertension in children. The hereditary and familial nature of VUR is now well recognized. The prevalence of primary VUR in the normal population is estimated at 0.5-2%. The prevalence of primary VUR in asymptomatic siblings, on the other hand, ranges between 4.7% and 50%. The incidence of renal damage in the siblings of patients with primary VUR is estimated as 3%- 41% (1). Course of the VUR is asymptomatic in most children. UTI may be the only sign that a child is at risk for VUR. This result justifies the usefulness of screening for VUR in the risk groups, particularly in the asymptomatic siblings of affected children. Previous reports have suggested that only siblings younger than 5 years of age would benefit from screening cystography (2). There is no consensus as to whether all siblings should be screened for reflux. The purpose of this study was to investigate the incidence and severity of VUR in siblings by means of ultrasonography (US), voiding cystourethrography (VCUG) and renal 99m technetium (Tc)-dimercaptosuccinic acid (DMSA) scintigraphy. MATERIAL AND METHODS From January 1994 to December 2005, we prospectively screened 71 siblings of 56 eligible index patients with VCUG as soon as the VUR of the index case was diagnosed, irrespective of the presence of symptoms and/or history of documented UTI. All children within this group had primary reflux. Siblings with structural abnormalities such as neurogenic bladder, posterior urethral valves, ureterocele or other congenital anomalies were excluded from the study. The patient population consisted of 32 boys and 39 girls. The mean age was 8.38±3.95 years (9 months to 15 years). Siblings were grouped into two, in order to observe the relation between age incidence and the severity of VUR. Siblings aged less than 6 years were included in the first group and siblings aged over 6 years were grouped in the second. The first group constituted of 39.4% (n=28) of all siblings, whereas 60.6% (n=43) of the siblings were in the second group. The age, gender, voiding pattern, urinary tract infection and past medical history, somatic growth rates, blood pressure levels, and urine culture results of the siblings were evaluated. BUN and creatinin levels were determined and VCUG and renal US examinations were performed to all siblings. Diagnosis of VUR was made by VCUG. The degree of VUR was evaluated according to international reflux study groups’ scale (3). All renal US were performed prior to the VCUG by the same experienced radiologist. The kidneys were studied by US for size, shape, parenchymal echogenicity, corticomedullary differentiation, irregularity of the kidney outlining and parenchymal reduction. DMSA renal cortical scintigraphy was performed in siblings with VUR to search for renal scars. Prior to the investigation, the nature, aim, potential risks, and benefits of VCUG and DMSA scans were explained to the parents and informed consent was obtained. RESULTS Seventy-one siblings of the 56 index patients were included in the study; 15 index patients were boys and the remaining 41 were girls. The age of the index patients ranged from 2 months to 12 years (5.4±3.1). Reflux was bilateral in 21 and unilateral in 35 index patients. The siblings group consisted of 32 boys and 39 girls with a mean age of 8.5±4.3 (9 months-15 years, Table 1). VUR was observed in 10 of 71 siblings (14%) with a mean age of 8.9 ± 4.3 years (3-15 years). Male to female ratio was found 3/7. UTI was found in 5 of the siblings with VUR. One of them had diurnal enuresis and another had nocturnal enuresis history. The rest of the siblings did not have any significant medical history. Furthermore, BUN and creatinin levels, and weight and height percentiles of siblings with VUR were found in normal ranges for their age. VUR was unilateral in 5 and bilateral in 5. VUR was found in 15 renal units in 10 patients, when a single kidney accepted as one renal unit. Of the 5 siblings with unilateral reflux, 3 had grade 2 and 2 had grade 3 reflux. Of the 5 siblings with bilateral reflux, one had bilateral grade 2, one had bilateral grade 3, one had grade 4 on the right side and grade 3 on the left side, one had grade 4 on the right and grade 5 on the left side, and one had grade 2 on the right and grade 4 on the left side. When the degree of VUR was compared between siblings aged less than 6 years and the siblings aged over 6 years, grade I-III VUR was found in 4 (26.6%) renal units in group I, and in 7 (46.6%) renal units in group II. On the other hand, grade IV-V VUR was found in 2 renal units (13.3%) in group I, and in 2 renal units (13.3%) in group II (Table 2). Of the siblings with VUR, 6 had normal kidneys on US and renal pathologies were evident in 4 of them. DMSA renal cortical scintigraphy was performed to the 10 siblings with VUR in order to search for renal scar. DMSA was normal in 5 cases. Of this group, 2 siblings had positive urine culture, but only one was symptomatic (nocturnal enuresis), the remaining did not have any symptom. Five siblings showed abnormalities, i.e. 2 asymmetrical differential functions and 3 parenchymal defects. Of the 5 siblings with abnormal DMSA scans, 4 were over 6 years of age and one was under 6 years. Of this group, 3 siblings had positive urine culture, but only one was symptomatic (diurnal enuresis). Of the 10 siblings with VUR, DMSA findings were abnormal in 5 and US findings were abnormal in 4 of the siblings. DISCUSSION Familial occurrence of primary VUR is a generally recognized problem (4). Autosomal dominant inheritance model with incomplete penetration and variable expression is currently being discussed. It supports the usefulness of screening, particularly among the affected patients’ siblings (5-8). The incidence of VUR in siblings of children with VUR is reported between 4.7-50% (4, 9, 10, 11), varying with age, gender, the presence of urinary tract infection symptoms and race (1, 2, 4). Nevertheless, the incidence of VUR in healthy children is less than 1% (12-16). In the present study, VUR was found in 10 of the 71 siblings. The incidence of VUR in siblings in previous studies was reported as 27% by Wan et al. (17) and 51% by Parekh et al. (18). Hollowel and Greenfield (19) have found the incidence of VUR in siblings as 32% in their study and the incidence was found 42.5% by Ataei et al. (20). The age of the sibling plays an important role in VUR development (18). The mean age of the 10 siblings with VUR included in the present study was found 8.9 ± 4.3 years, whereas the incidence of VUR was found 14%, which was nearly equal to the lower limit of the incidence of VUR reported in the literature. This might be due to the higher mean age of the siblings in the present group, since the incidence of VUR decreases with the increase of the age. In Hollowel and Greenfield’s study (19), the mean age of the siblings was found 6.2 years, where the frequency of VUR was found as 27%. However, in another study, the mean age was found 2.8 years and the frequency of VUR was found as 37% (17). Most authors reported that siblings over 5-7 years suffer from reflux considerably less often (1, 17). In the present study, we found the frequency of VUR as 14.2 % in the siblings under the age of 6 years, whereas the frequency of VUR in the group of siblings aged over 6 years was found 13.9%. Wan et al. (17) and Connolly et al. (1) stated the frequency of VUR in siblings over 6 years as 4.7 and 7%, respectively. In the study of Noe (21), the frequency of VUR was found 28% in children aged over 6 years, and 32% in children aged less than three years. In the presented study the frequency of VUR in both groups were found nearly the same. When the degree of VUR is evaluated in two different age groups, grade I-III VUR was found in 4 renal units (26.6 %) in the first group, which consisted of siblings aged less than 6 years. On the other hand, grade I-III VUR was found in 7 renal units (46.6 %) in the second group, including siblings aged between 6 and 20 years. Grade IV-V VUR was found in 2 (13.3 %) renal units in the first group. Likewise, grade IV-V VUR was found in 2 renal units (13.3%) in the second group. In siblings with VUR the frequency of grade I-III VUR was higher. In total, grade I-III VUR was found in 73.3 % and grade IV-V VUR was found in 26.6 % of all siblings with VUR. Grade I-III VUR was found in 95% of all siblings with VUR in the study by Wan et al. (17). Kuczynska et al. (4) stated the frequency of grade I-II VUR as 88.9%. Eventually, we found the frequency of grade I-III VUR higher than grade IV-V, although this is less than the results reported in the literature. To rule out renal scars, DMSA was performed to 10 siblings with VUR. One or more renal scars were found in 5 (50%) of these siblings. Positive urine culture was present in 3 of them, but only one had urinary symptom. Of the 5 siblings with abnormal DMSA scans, 4 were over 6 years of age and one was less than 6 years. The grade of VUR was found to be grade III or higher in siblings with renal scar. The most important and severe complication of VUR is renal parenchymal scar. Some other causes, including intrarenal reflux due to high pressure, infectious diseases, and immune mechanisms are also accused of renal scar development (13, 14, 22, 23). The ratios of renal scars in siblings were found between 5% and 20% in four previous studies (17, 21, 24, 25). In our study, the ratio of renal scar was found higher than those reported in literature. So we recommend that a DMSA scan should be performed after VCUG in siblings with reflux. Urinary tract infection history was not present in most of the siblings with VUR. This data shows that renal scars may not have infectious origin, but may be a result of congenital dysplasia or high degree of reflux (19). Two of the siblings included in our study had renal scars without any urinary tract infection history. Though ultrasonography was performed to all siblings, 60% of the siblings with VUR had no pathologic findings on ultrasonography. As stated in literature, this data shows that ultrasonography is not a sufficient diagnostic tool for showing VUR. Blane et al. (26) reported that ultrasonography did not detect any pathology in 73.9 % of patients with VUR, but only pyelocaliectasia in 26.1% of these patients. Kenda et al. (27) did not find any pathology with ultrasonography in siblings of affected patients. This data confirms that ultrasonography is not a sufficient diagnostic tool for detection of VUR in siblings. In conclusion, according to our study, the risk of VUR in siblings of affected patients is higher than the normal pediatric population. We did not observe any significant difference in the frequency of VUR between the siblings aged less than 6 years and the siblings aged over 6 years in our study. Furthermore, in the present study, diversely from the literature, high grade VUR was detected in siblings aged over 6 years, so it is recommended that all siblings over 6 years or less than 6 years should be evaluated for VUR. Eventually, we think that the parents of children with VUR should be informed about the incidence of this entity in siblings aged less than 15 years. Also, the benefits of investing these siblings should be stressed. One should not forget that the incidence of reflux nephropathy in asymptomatic siblings decreases with early diagnosis and treatment. Since ultrasonography is not sufficient for diagnosis, a noninvasive and effective diagnostic method, instead of conventional voiding cystouretrography, is needed. REFERENCES
Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08017t2.jpg] [gm08017t1.jpg] |
| |||||||||

{kind=link}
{kind=link}