 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
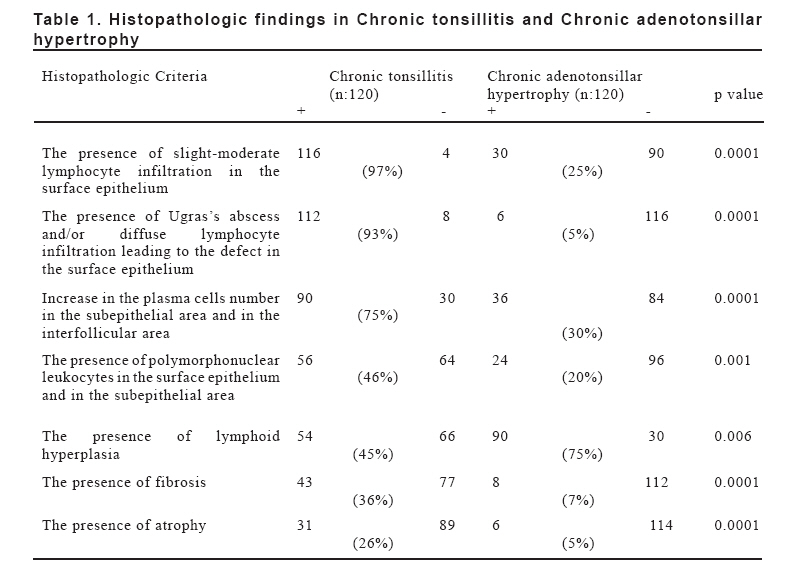
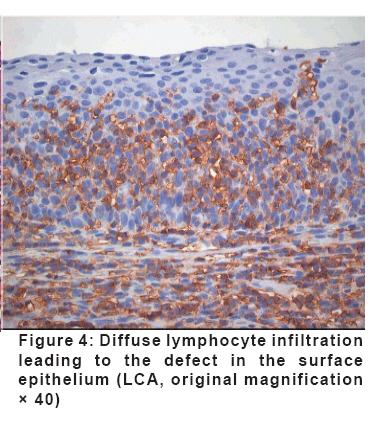
European Journal of General Medicine, Vol. 5, No. 2, 2008, pp. 95-103 Chronic Tonsillitis Can Be Diagnosed With Histopathologic Findings Serdar Uğraş1, Ahmet Kutluhan2 Ankara Ataturk Education and Research Hospital, Departments of Pathology1 and Otorhinolaryngology2, Ankara, Turkey Code Number: gm08018 Aim: The objective was to identify histopathologic findings of the chronic tonsillitis in the palatine tonsils.
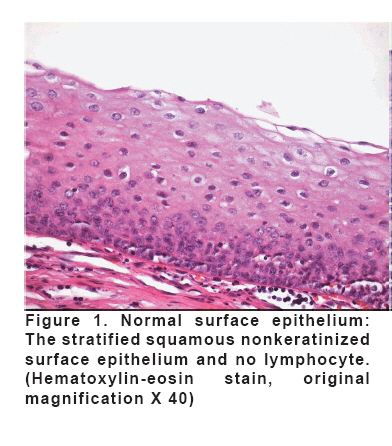
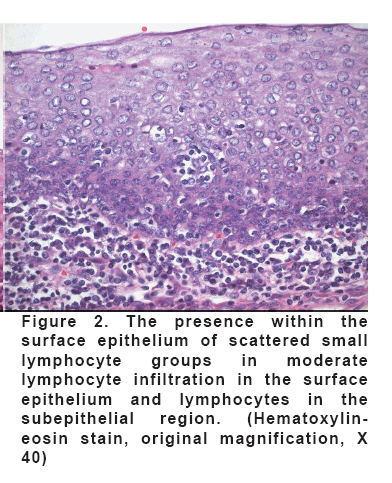
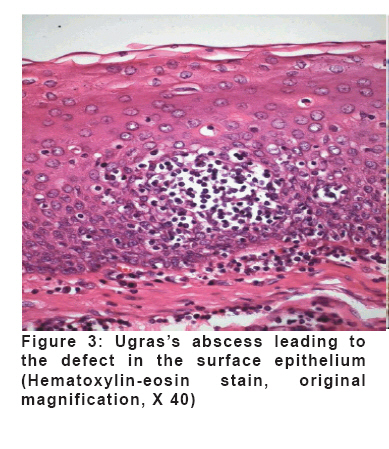
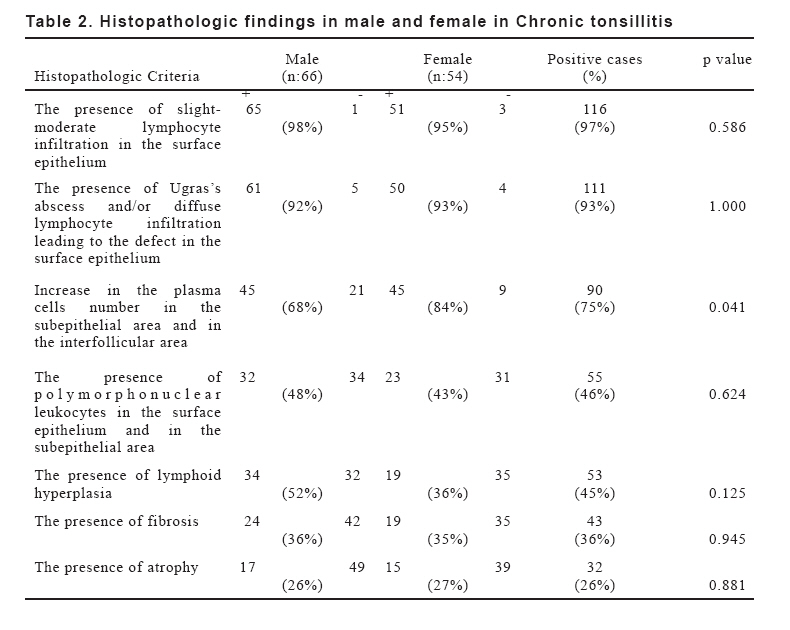
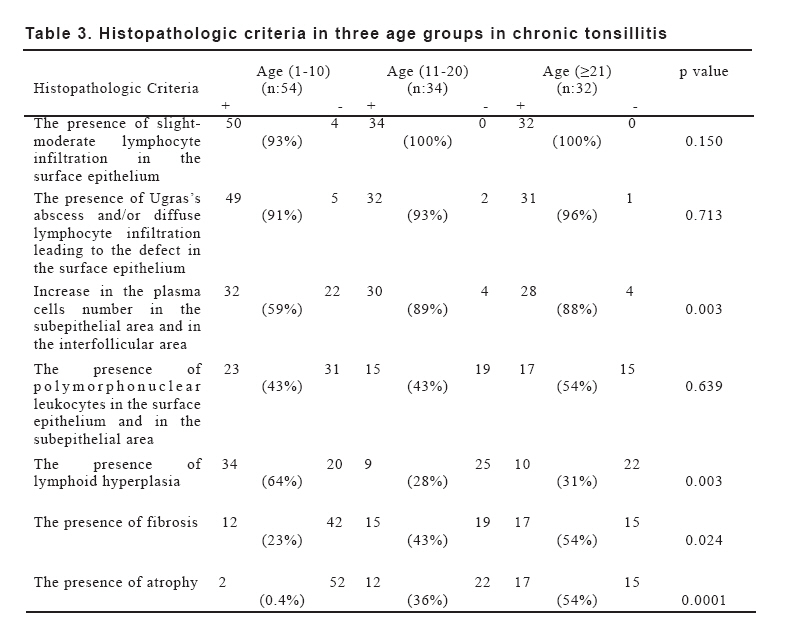
Key words: Chronic tonsillitis, diagnosis, pathology, tonsillectomy, palatine tonsil INTRODUCTION Tonsillar diseases are among the most commonly encountered health-related problems in the general population. The choice of treatment is often tonsillectomy, which is still the most frequently performed surgical procedure in children and young adults. Although chronic tonsillitis are still the most common reasons for tonsillectomy (1), histopathological criteria for this infection have not been well studied. All investigations were confined to the lymphoid follicle, germinal centre and crypts, rather than investigating the changes in the entire tonsil area including surface epithelium (1-8). Thus the results from these studies have been inconclusive. To our knowledge, specific and reliable histopathologic criteria of the chronic tonsillitis had not been described in English literature up to now. Therefore, we aimed to identify significant histopathological criteria of the chronic tonsillitis in the palatine tonsils on selected patients. MATERIALS AND METHODS This study was performed on a total of 120 patients (66 males, 54 female, mean age 16 years, range 4 to 48 years) with chronic tonsillitis and a total of 120 patients (60 males, 60 female, mean age 9 years, range 2 to 17 years) with chronic adenotonsillar hypertrophy. Patients or their parents were asked about a history of recurrent tonsillitis or previous admission to hospital due to tonsil infection. On physical examination, the presence of hyperaemia on the anterior pillars, crypt debris, intratonsillar abscess, peritonsillar abscess, hypertrophy and asymmetry of the tonsils were examined. Patients with chronic tonsillitis were those who had more than six episodes per year or three episodes per year for ≥ 2 years with tonsillar hypertrophy and hyperaemia on the anterior pillars. Diagnosis of chronic tonsillitis was based on history and physical examination. Patients with obstructive sleep apnea, peritonsillar abscess or recent acute tonsillitis were excluded from this study. Bilateral tonsillectomy was performed in all 240 patients under general anaesthesia or under local anaesthesia. The palatine tonsils were fixed in 10 % neutral-buffered formalin for a day. Then four tissue pieces (1x1x0.5cm in diameter) including surface epithelium obtained from each palatine tonsil. Four-micrometer-thick serial sections were cut and stained with hematoxylin-eosin. In addition, Masson’s trichrome stain was performed to verify fibrosis in the subepithelial region. Immunohistochemically, CD3 for T lymphocytes (PC3/188A, DAKO), CD20 for B lymphocytes (L26, DAKO) and LCA (2B11+PD7/26, DAKO) were performed to identify the lymphocytes in the surface epithelium and crypt epithelium of the palatine tonsil. In addition, Cytokeratin (0053A, DAKO), Cytokeratin, LMW (0059I, DAKO) and Cytokeratin, HMW (0090G, DAKO) were performed to identify defect in the surface epithelium and crypt epithelium. Eight histopathologic criteria were investigated all palatine tonsils: 1-the presence of slight-moderate lymphocyte infiltration in the surface epithelium (SMLI). a-The presence of slight lymphocyte infiltration in the surface epithelium is characterized by the presence, within the surface epithelium of the tonsil, of scattered single lymphocytes more than a very few, often surrounded by a halolike clear space. b-the presence of moderate lymphocyte infiltration in the surface epithelium is characterized by the presence, within the surface epithelium, of scattered small lymphocyte groups. 2-the presence of abscess leading to the defect in the surface epithelium (Ugras’s abscess). Ugras’s abscess consist of small or large intraepithelial groups of often tightly aggregated lymphocytes located within a vacuole. Microvesiculation can also be observed. 3-the presence of diffuse lymphocyte infiltration leading to the defect in the surface epithelium (DLI). 4-the presence of polymorphonuclear leukocytes in the surface epithelium and in the subepithelial area (PL). 5-the presence of lymphoid hyperplasia (LH). 6-increase in the plasma cells number in the subepithelial area and in the interfollicular area (IPCN). 7-the presence of fibrosis (F) 8-the presence of atrophy (A). The statistical analyses was performed by t-test, chi-square test and Fisher’s exact test. Probability levels of less than 0.05 were considered significant. RESULTS A total of 240 patients were included in this study. In chronic tonsillitis group, there were sixty-six (55%) male and fifty-four (45%) female patients. The mean age was 16 years with a range of 4 to 48 years. The preoperative diagnosis was chronic tonsillitis in all patients. In chronic adenotonsillar hypertrophy (CAH) group, there were sixty (50%) male and sixty (50 %) female patients. The mean age was 9 years with a range of 2 to 17 years. The preoperative diagnosis was CAH in all patients. All histopathologic criteria showed a statistically significant difference (p=0.0001) between chronic tonsillitis and chronic adenotonsillar hypertrophy. Although seven criteria were more closely associated with chronic tonsillitis, only one criteria (the presence of lymphoid hyperplasia) was higher in chronic adenotonsillar hypertrophy compared chronic tonsillitis (p=0.0001) (Table 1). In chronic tonsillitis group, there was no statistical difference in between male and female with regard to presence of histopathologic criteria except for plasma cells. IPCN was more common in females (p< 0.041). Histopathological examination showed SMLI (Figure 1,2) and the presence of Ugras’s abscess (Figure 3) and/or DLI (Figure 4) in 98, 92 and 95, 93 % in male and female, respectively. Other findings were observed between 26% and 68%, except for IPCN in female (84%) (Table 2). In chronic tonsillitis group, there was statistical differences among three groups with regard to presence of histopathologic criteria. Histopathological examination showed increased LH presence in 1-10 age group statistically, compared to the other groups (p=0.003). We observed IPCN, F and A were lower in 1-10 age group statistically, compare to the other groups and p values were, p=0.003, p=0.024, p=0.000, respectively. Histopathological examination showed SMLI in 93 and 100 % before and after 10 years of age, respectively. The presence of Ugras’s abscess and/or DLI were seen in 91 and 95% before and after 10 years of age, respectively. The presence of PL, F and A were higher after 21 age group compared to 1-20 age group (Table 3). Immunohistochemically, strong staining for CD20 (B cell antigen) antibody and LCA antibody were observed on the lymphocytes in the surface epithelium and in the crypt epithelium and in the lymphoid tissue of the palatine tonsil. These antibodies were also observed on the lymphocytes in crypt epithelium and in the lymphoid tissue of the palatine tonsil. Staining with CD3 antibody was negative on the lymphocytes in the surface epithelium and crypt epithelium except for only a few lymphocytes. Defect in the surface epithelium and crypt epithelium was observed with Cytokeratin antibody, very well. DISCUSSION Chronic tonsillitis, is a disease with relapsing and remitting acute attacks or a subclinic form of a resistant infection, a poorly treated kind (9). It is impossible to differentiate chronic tonsillitis from recurrent tonsillitis and these two terms were used to represent the same disease process. Only if a patient’s tonsils returned macroscopically and histologically to normal between episodes could recurrent tonsillitis be differentiated from chronic tonsillitis (2). Slight-moderate lymphocyte infiltration and the presence of Ugras’s abscess and/or diffuse lymphocyte infiltration leading to the defect in the surface epithelium not present in normal tonsils. Therefore, combination of three findings are fairly diagnostic for chronic tonsillitis. These findings are present in 97 and 93% in chronic tonsillitis, respectively. But these findings are present in 25 and 5% in CAH, respectively. The current indications for tonsillectomy are usually chronic infectious conditions such as chronic tonsillitis or chronic upper-airway obstruction in conjunction with tonsillar hypertrophy (10). The diagnosis of the chronic tonsillitis is important and the effect of tonsillectomy on the patient’s immunological integrity are widely debated (1). In the past 100 years one of the most important indications for removal of the tonsils was chronically inflamed tonsils. Recently, there has been a strong reaction against the operation, pointing out the lack of sound scientific basis (11), especially with the growing knowledge of the immunological functions of the tonsils. As a route of pathogen entry, the tonsils are well known for postviral infection with bacteria (12) and also the Epstein–Barr virus (13). However, even today, tonsillitis is known to play an important role in the occurrence of secondary diseases in the form of focal infection such as IgA nephropathy (14) , arthropathy (15) and reactive arthritis (16). All of these diseases have in some cases improved after tonsillectomy. The healthy palatine tonsils are sites of continuous stimulation of lymphoid cells and this has been interpreted as a permanent activation (17). Up to now only few systematic studies exist, comparing recurrent or chronically inflamed tonsils with “normal” ones (18). Tonsillitis occurs if the activity and proliferation of pathogens in the tonsillar lymphoid tissue exceed the protective potency of activated lymphoid and immunoglobulin-producing cells (19). In this situation, especially in chronic or recurrent cases, surgical tonsillectomy is a common therapeutic approach (20), but is still controversial (21,22). It remains unclear whether its benefit exceeds its harm, i.e. the elimination of enormous numbers of immunocompetent cells occasionally resulting in a decreased level of serum IgA (23-25). Furthermore, it has to be taken into consideration that large palatine tonsils alone are not necessarily an indication for tonsillectomy, because tonsils are normally much larger in children than in adults and physiologically involute during adolescence (26,27). Although an accurate number of episodes is often difficult to obtain in some region of the world the diagnosis of the chronic tonsillitis is usually based on clinical history. At least three or more episodes in each of the three preceding years despite adequate medical therapy can be accepted as clinical criterion of the chronic tonsillitis and as an indication for tonsillectomy (28). Seven or more episodes in the preceding year or five or more episodes in each of the two preceding years be accepted as clinical criterion of the chronic tonsillitis and as an indication for tonsillectomy (29). Despite the prevalance of chronic tonsillitis and tonsillectomy, relatively few studies have investigated the impact of the histopathologic diagnosis of the chronic tonsillitis. Unfortunately these studies were confined to the lymphoid follicle, germinal centre and crypts, but the entire tonsil area including surface epithelium has not examined in these studies. Friedmann suggested that the principal features of the chronic tonsillitis are lymphoid hyperplasia, distension of the crypts and fibrosis of the parenchyma (3). Bieluch et al found that chronic cryptitis, various degrees of lymphoid hyperplasia and intact tonsillar architecture in tonsils from patients with chronic tonsillitis (2). Woodruff found same findings as an exuberant cryptitis and intact tonsillar architecture (4). Wright and Alvi also found same findings as cryptitis and lymphoid hyperplasia in tonsils from patients with chronic tonsillitis (5,6). In the palatine tonsils of the healthy person, the epithelia lining the crypts are infiltrated with nonepithelial cells (mainly lymphocytes), and are underlined with disrupted basement membrane but no thick connective tissue band. The degree of reticulation and lymphocytic infiltration is pronounced in the palatine tonsils (30). Therefore, histopathologic criteria as cryptitis and chronic cryptitis should not be used as chronic tonsillitis criteria. Using the point counting method, Surjan estimated germinal centre size and concluded that germinal centres were enlarged in hypertrophic tonsils compared with those from patients with chronic tonsillitis (7). Gorfien et al used image analysis to measure germinal centre size and found that there is a significant increase germinal centre area in hypertrophic tonsils from patients with recurrent tonsillitis or with tonsillar hypertrophy compared with normal controls (8). Zhang et al also used image analysis to estimate follicle numbers and follicle area. They concluded that there was no significant difference in the mean follicle numbers between recurrent tonsillitis and tonsillar hypertrophy, however, the mean follicle area in the tonsillar hypertrophy group is significantly larger than in the recurrent tonsillitis group, and therefore that tonsillar hypertrophy is characterized histologically by an enlargement of follicles (1). We think lymphoid hyperplasia is a nonspecific finding, which may be seen in tonsillar hypertrophy, acute tonsillitis and chronic tonsillitis in the palatine tonsil. Therefore this finding should not be used as only the chronic tonsillitis criteria. Because lymphoid hyperplasia is enlargement of lymphoid organs as a consequence of hyperplasia of some or all of the cellular components, reflecting stimulation of the lymphoid cells by a variety of antigens or allergens (31). We examined inflammatory cell infiltration in the surface epithelial cells of the palatine tonsils. Because in the pathology textbooks, infiltration of epithelial cells by benign inflammatory cells has been used as a criteria for inflammation (e.g. cholangitis, lymphocytic colitis, active chronic gastritis, spongiform pustule of Kogoj in Psoriasis). The palatine tonsils are covered with stratified squamous nonkeratinized epithelium. This epithelium is avascular and only a very few nonepithelial cells are found here in normal healthy person (30). In chronic tonsillitis group, we observed SMLI, Ugras’s abscess and/or DLI in the surface epithelium. SMLI and Ugras’s abscess and/or DLI were present in almost all of the patients in every age group and both sex, and in the groups with 3-5 attacks or in the patients with 6 or more attacks. Therefore, these three findings are a very helpful and reliable diagnostic features to diagnose chronic tonsillitis histopathologically. The presence of one of these criteria is not enough to diagnose chronic tonsillitis. We believe least two of three findings can be seen all of cases of the chronic tonsillitis, particularly if several tissue specimens were examined. We demonstrated numerous lymphocytes in the lymphoepithelium, and degenerated cells and cellular debris in the crypts. We did not diagnose chronic tonsillitis with these findings which can be seen in healthy population. It is important to differentiate surface epithelium and crypt epithelium. Because it may be difficult to differentiate since surface epithelium may show diffuse lymphocyte infiltration. In that case it is necessary to evaluate basal membranes and subepithelial thick connective tissue band. Although crypt epithelium is underlined with disrupted basement membrane but no thick connective tissue band, surface epithelium is underlined with normal basement membrane and there is a thick connective tissue band in subepithelial region. Plasma cells are predominantly located around intraepithelial capillaries in the palatine tonsil (32). Therefore we examined plasma cells outside of this location and in subepithelial area and interfollicular area especially. Histopathological examination have shown the presence of IPCN, F and A statistically is low and LH is high in the patient over 11 years or older compared to the patients 1-10 years (p<0,003, p<0,024, p<0,000 respectively). This has caused chronic inflammation in the tonsils, decrease in lymphoid tissue, fibrosis and atrophy which eventually migration of more chronic inflammatory cells to the tissue. This is same in any chronic nonspesific inflammation in any part of the body. This result also show that atrophy and fibrosis is related to frequent attacks or a long time chronic infection. Besides involution causes increase A and F and decrease in LH in patients over 10 years-old. Tonsils are normally much larger in children than in adults and physiologically involute during adolescence (26,27). Therefore, in physical examination, atrophic and/or fibrotic tonsils can be expected in patients with chronic tonsillitis over 10 years old. In chronic infection as chronic tonsillitis, the circulation of blood is poor as a result of degenerative changes causing parenchymal fibrosis. In contrast, tissue hyperplasia and vessel proliferations occur when the palatine tonsils become hypertrophic (33). Ozdemir et al found that a statistically significant decrease in blood flow in chronic tonsillitis and a significant increase in hypertrophic tonsils compared to the normal controls (34). These observations and our result indicate that systemic antibiotics may have insufficient effect in patients with chronic tonsillitis over 10 years old. In conclusion, it is not safe to depend on the attack number to diagnose chronic tonsillitis. Because chronic tonsillitis can be diagnosed in patients with fewer than three episodes in each of the three preceding years or in patients with fewer than five episodes in each of the two preceding years or in patients with fewer than seven episodes in the preceding years. Furthermore, chronic tonsillitis can be diagnosed in patients with fewer than two episodes in the preceding years. When the diagnosis of chronic tonsillitis performed with the criteria described in this study on punch biopsy performed before tonsillectomy procedure: a-Diagnosis may be true before surgery. b-Tonsillectomy may not be performed in unnecessary and wrong diagnosis cases. c-When the diagnosis is chronic tonsillitis in punch biopsy specimen tonsillectomy may be performed to prevent chronic tonsillitis complications. REFERENCES
Abbreviation: SMLI: The presence of slight-moderate lymphocyte infiltration in the surface epithelium, DLI: The presence of diffuse lymphocyte infiltration leading to the defect in the surface epithelium, PL: The presence of polymorphonuclear leukocytes in the surface epithelium and in the subepithelial area, LH: The presence of lymphoid hyperplasia, IPCN: Increase in the plasma cells number in the subepithelial area and in the interfollicular area, F: The presence of fibrosis, A-The presence of atrophy, CAH: Chronic adenotonsillar hypertrophy Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08018f2.jpg] [gm08018f3.jpg] [gm08018t2.jpg] [gm08018f4.jpg] [gm08018t1.jpg] [gm08018f1.jpg] [gm08018t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}