 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
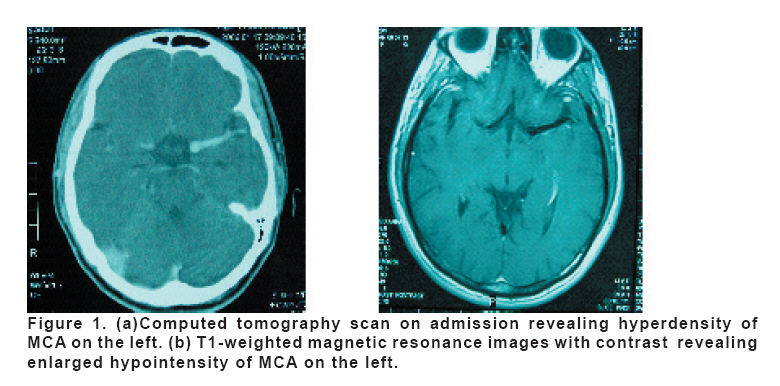
European Journal of General Medicine, Vol. 5, No. 2, 2008, pp. 115-117 Complete Isolated Third Nerve Paresis Assosicated With Fusiform Dilatation Of Middle Cerebral Artery Abdulkadir Koçer and Şefika Okuyucu Düzce University, School of Medicine, Department of Neurology, Düzce, Turkey. Code Number: gm08022 A 28 year-old-male sufferred left third nerve paresis. A pattern of complete and isolated paresis was observed. Neuroimaginings and conventional cerebral angiography revealed abnormally enlarged middle cerebral artery. Because of its fusiform nature, the abnormality was left untreated surgically. The third nerve palsy began to resolve within a week from onset after prednisolone administration. The present case was interesting because of resulting from fusiform dilatation of middle cerebral artery which was the only finding related to the third nevre palsy and early recovering of pupil. Key words: Third nerve paresis, fusiform, aneursym, pupil, middle cerebral artery INTRODUCTION Third nevre palsy (TNP) can result from lesions located anywhere from the oculomotor nucleus to the termination of the third nerve in the extra-ocular muscles. Basilar portion which extends from brain stem to cavernous sinus is the most important part and the most commonly seen anerusyms are posterior communicating artery related (1). New and recent advances in neuroimaging makes diagnosis easy; however, management of a patient presenting with an isolated third nerve palsy remains a challenge. CASE A 28 year-old-man was admitted to our hospital because of sudden onset of ptosis and diplopia developped within last two days. On admission, the patient was alert and had no neurological deficit except for left third nerve paresis (TNP). The left eye showed ptosis with complete absence of adduction. The left pupil was 6 mm in diameter and nonreactive to light; the right pupil was 3 mm in diameter. The indirect light response on the left was present. Cranial Computed Tomography revealed hyperdense and dilated middle cerebral artery (MCA) on the left side. Magnetic resonance imaging (MRI) and angiography demonstrated a fusiformly dilated MCA in compare to right side (Figure 1). Cerebral angiography revealed the fusiform enlargement of MCA which was extented from the internal carotid artey bifurcation to the left MCA M1 segment and the inferior branch. Routine biochemical and microbiological blood examinations, serum levels of ESR, B12, folate, protein C, protein S, ASO, CRP, RF were normal. Tests related to hepatitis and thyroid hormone functions revealed normal results. Lyme, Anti-cardiolipin, Anti-nuclear, Anti-DNA and Anti-HIV antibodies were negative. CSF analysis was normal. No systemic abnormality predisposing to aneurysms or dilatation was found. Because of its fusiform nature, the abnormality was left untreated surgically. Prednisolone (1 gr/daily) was administered for five days. The third nerve palsy began to resolve within a week from onset, and by one month the ptosis and ophthalmoparesis had improved markedly. At 3-month follow-up he had a complete recovery clinically. DISCUSSION Acquired TNP may be partial or complete, isolated or accompanied by signs of more extensive neurological involvement. The diagnosis and management varies according to the age of the patient, characteristics of the third nerve palsy, and presence of associated symptoms and signs (1,2,7). Acquired, isolated TNP is actually a manifestation of an intracranial cerebrovascular pathology. Complete TNP occurring in isolation are often due to compressive lesions or meningeal infiltration thus a MR scan is needed. If this study is negative, a cerebral angiogram is necessary to investigate aneurysm or dural-cavernous sinus fistula. If meningeal signs are present, spinal fluid evaluation is warranted. A fully dilated and non-reactive pupil occurs in up to 71% of patients with aneurysmal compression and TNP(1,4-6). Our patient was presented with an isolated complete TNP and did not have any additional clinical findings i.e. motor and sensory findings, ataxia, other cranial nerve pathologies. We thought that it was resulted from extraaxial abnormality. He was examined by computed tomography, and then cranial MRI and MRI angiography (Figure 1a and b, Figure 2). A vascular abnormality was noted on MRI. This procedure was followed by conventional cerebral angiography. There was a clinical evidence to indicate that a case of compressive cerebral aneurysm causing the isolated third nerve palsy but angiography showed only fusiformly enlarged MCA on the left side (Figure 3). Isolated, acquired TNP atributable to MCA abnormalities are extraordinarily rare although lots of reports atributable to posterior communicating aneurysms or posterior circulation (1-5,7). There are some large report series of patients with TNP and they report that MCA aneurysms may be associated with TNP (3,6,7). A complete TNP resulting from an intracranial fusiform dilatation of MCA could not be found in a MEDLINE search. Another important point that pupil response was the first sign of recovery in our patient. He had no history of diabetes and did not say about eye pain accompaning nerve ischemia. There was no radiological evidence of brain stem or nerve root exit patholgy. He showed a pupil-sparing paresis after one week of therapy, which is not common with traumatic damage or aneurysms. In summary, our case was interesting because we did not find any inflammatory or infectious condition to explaine the complete TNP. Complete TNP of resulting from fusiform dilatation of MCA and early recovering of pupil has not been previously reported, and the temporal relationship of the MCA fusiform aneursym to the TNP neuropathy is compelling, although not definite, evidence of a causal relationship. REFERENCES
Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08022f3.jpg] [gm08022f2.jpg] [gm08022f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}