 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
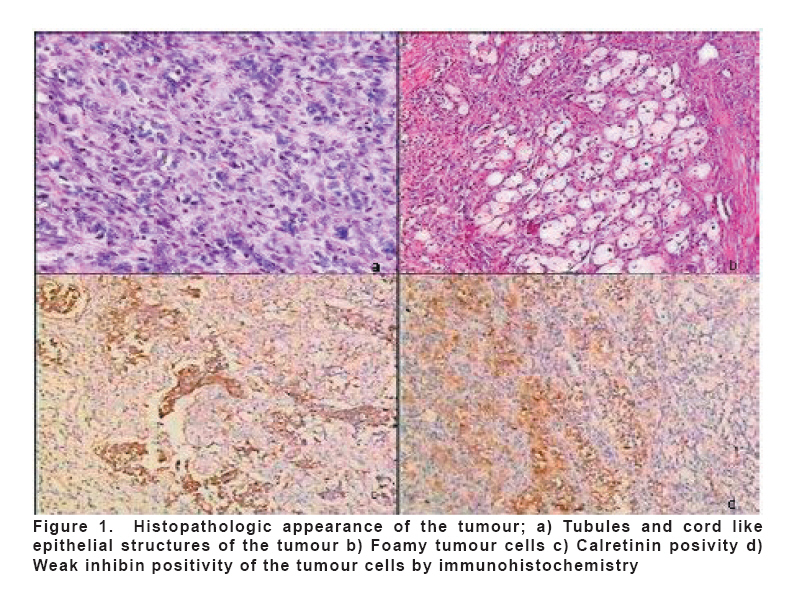
European Journal of General Medicine, Vol. 5, No. 2, 2008, pp. 118-120 Uterine Tumour Resembling Ovarian Sex Cord Tumour Murat Dede1, Kazım Gezginç1, Müfit C Yenen1, Mustafa Ulubay1, Mükerrem Safalı2, İskender Başer1 Gulhane Military Medical Academy, Departments of Obstetrics and Gynecology1 and Pathology2, Ankara, Turkey. Code Number: gm08023 To present a rare case which was resembling ovarian sex cord tumours. A 37 year old woman who had vaginal bleeding for three months was admitted to our clinic. An intracavitary mass was detected after the saline infusion sonography. The patient had operative hysteroscopy. A submucosal mass was resected with hysterescopic knife and resectoscope. According to pathology report, the tumour was diagnosed as uterine tumour resembling ovarian sex cord tumour (UTROSCT) infiltrating half of the myometrial wall. Then a thorough systemic evaluation was performed in order to detect any metastatic lesions. After evaluation of all systems, total abdominal hysterectomy and pelvic-paraaortic lymph node sampling was performed. All the diagnostic and therapeutic procedures were done in our clinic. There are no common consensus for approaching to these patients, these tumours are so rare and clinical features are so variable. Extensive studies must be performed about these tumours. Key words: Uterine Tumour, Ovarian Sex Cord Tumour, Clinical Features, Management. INTRODUCTION Endometrial neoplasms resembling ovarian sex cord tumours are very rare with less than 100 documented cases in the literature. Morehead and Bowman (1) first described uterine tumour resembling ovarian sex cord and stromal tumours in 1945. In their review in 1976, Clement and Scully (2) described 14 cases classified into two groups based on clinical and histological features. In the first group, differentiation rate for endometrial stromal tumours into sex cord like aggregates were less then 50% and in the second group, tumour consisted of almost sex cord like components. In the first sight, two groups seemed to be similar but clinical features of the disease was actually different (2). These tumours are treated with simple hysterectomy usually. In our case, we also added pelvic-paraaortic lymph node sampling to the procedure. The literature describing the clinical features and management of these tumours are limited with a few articles, but hysterectomy is still the most common procedure for the management. We have approached to this case as an ovarian sex cord stromal tumour and performed staging laparatomy procedure. CASE A 37 year old Gravida 2, Para 1, Abortion 1 woman complaining of vaginal bleeding for three months was admitted to our clinic. The patient had no surgical operation or previous medication for any diseases before. In physical examination, no remarkable finding had been found. In pelvic examination; the uterus was in normal size, antevert in position and mobile, no adnexial masses were found. Transvaginal ultrasound examination (TVUSG) was normal and endometrial curettage had been performed. Endometrial biopsy was reported as normal cytology. One month later, the patient was admitted for the same complaint and an intracavitary mass was detected after the saline infusion sonography. At first sight, it had been thought that this mass could be endometrial polyp. Then the patient underwent operative hysteroscopy. Submucosal mass was resected with hysteroscopic knife and resectoscope. Pathologic examination was as uterine tumour resembling ovarian sex cord stromal tumour. Imaging studies were performed for further evaluation. In TVUSG, endometrial irregularity was noticed with minimal free fluid in the Douglas pouch. Also, we studied thoracal and abdomino-pelvic CT scan. No metastatic or pathologic lymphadenopathy was reported. Bilateral breast ultrasonography showed minimal fibrocystic changes. Cervicovaginal smear was normal. Routine biochemistry, whole blood count, tumour markers and serum inhibin levels were in normal ranges. We have discussed the theraphy approach with the patient and she was consented for total abdominal hysterectomy. In the operation, we performed total abdominal hysterectomy and pelvic-para aortic lymph node sampling without any complications. Considering her age, we have preserved the ovaries. Macroscopic examination of hysterectomy revealed a polyploid and infiltrative tumour 3.5 cm in size located in the uterine fundus. Microscopically, tumour composed of epithelial like structures arranged in cords, trabeculae, nests and tubules resembling ovarian sex cord-like elements and was infiltrating myometrium (Figure 1a). Tumour cells were small and cuboidal in shape with scant eosinophilic cytoplasm and round to oval nuclei with indistinct nucleoli resembling those of the surrounding stromal cells. Some of the tumour cells were polygonal with pale and foamy cytoplasm, grouped as small nodules (Figure 1b). Nuclear atypia was mild and mitotic activity was low (one to two mitoses per 10 high-power fields). Immunohistochemical tests showed immunoreactivity in the tumour cells for cytokeratin, actin, calretinin (Figure 1c), CD99 and inhibin (weak) (Figure 1d). EMA was negative. Pathologic diagnosis was uterine tumour resembling ovarian sex cord tumour infiltrating half of the myometrial wall. Pelvic-para aortic lymph nodes were demonstrating reactive hyperplasia without metastasis. DISCUSSION For the preoperative assessment of abnormal vaginal bleeding endometrial curettage might be included in some cases. In our case, no abnormality had been shown in endometrial curettage except chronic endometritis. Preoperative diagnosis is difficult for this tumour. Because, it is rare and no abnormality can be seen in imaging studies. In one case, sonographic presentation of a polypoid mass was present within the endometrial cavity. This tumour was echogenic and mimicked an endometrial polyp (4). In our case, saline infusion sonography showed an endometrial echogenic polypoid mass. We also performed PET scan to our patient, which was normal. Positron emission tomography (PET) scanning utilizes the recognized tumour metabolic property of increased glycolysis with the radioactive decay of 2-[(18)F] fluoro-2-deoxy-D-glucose (FDG) and generation of gamma radiation to provide quantitative tumour imaging. According to our knowledge no studies within PET scan have been done for uterine tumour resembling ovarian sex cord tumours before; we performed PET scan to our patient and result was normal. Tumour markers like CA-125 and inhibin are less effective in detecting sex cord stromal tumours. Serum inhibin levels can be useful in granulosa cell tumours after menopause. Serum inhibin level was (61 mIU/ml) and normal in our case. In Clement and Scully’s classification, in the first group patients, three of six had recurrence tumours three years after the operation. In the second group patients, no recurrence were reported in 7 years follow up period (3). We have followed our patient for 9 months closely. We haven’t seen any postoperative complications and recurrence. All of the lymph nodes were reactive in pelvic paraortic lymph node sampling and peritoneal biopsies were normal. So according to our staging laparatomy procedure, we expect to see full recovery from our patient. Although the prognosis of these tumours are usually benign in the literature, we should not forget that these tumours may cause metastatic lesions due to malign transformation (5). There are no common consensuses for approaching to these patients, yet, these tumours are so rare and clinical features are so variable. Extensive studies must be performed about these tumours. REFERENCES
Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08023f1.jpg] |
| |||||||||

{kind=link}