 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
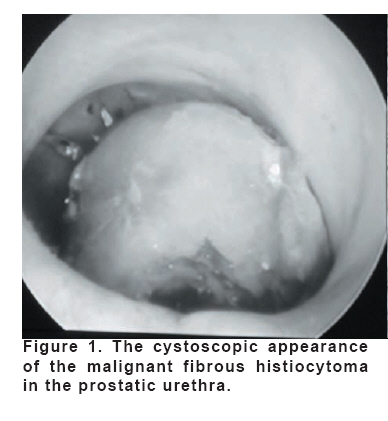
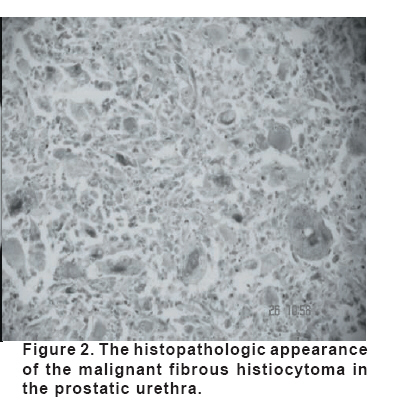
European Journal of General Medicine, Vol. 5, No. 2, 2008, pp. 123-125 Malignant Fibrous Histiocytoma Of The Prostate In The Prostatic Urethra Ahmet Gökçe1, Mehmet İnci2, Oğuz Ekmekçioğlu1 Erciyes University Medical Faculty, Department of Urology1, Kayseri State Hospital, Urology Clinic2, Kayseri, Turkey Code Number: gm08025 Malignant fibrous histiocytoma is a rare tumor of the prostate. We present an unusual case with malignant fibrous histiocytoma of the prostate in the prostatic urethra. The patient was treated with transurethral resection of the tumor. The postoperative metastatic work up was negative. Key words: Malignant fibrous histiocytoma, Prostate, Urethra INTRODUCTION Malignant fibrous histiocytoma of the prostate is a primitive mesenchymal tumor which rarely occurs in the prostate. It can be diagnosed in histopathological examination and is generally with prostate adenocarcinoma. Malignant fibrous histiocytoma of the prostate has been rarely reported as case reports or in case series of other sarcomas of the prostate (1-3). CASE A 72-year-old male presented with the complaints of hematuria and difficulty in voiding for five months. His physical examination revealed a little firm prostate. His testicles had been removed surgically for the treatment of prostate adenocarcinoma and had been given antiandrogen therapy. He had been diagnosed as prostate cancer following TUR-P one and half year ago. In histopathological examination the diagnosis was prostate adenocarcinoma with 5+3 gleason score. Before the first operation total PSA value was 18.25ng/ml. Because of the fact that his obstructive voiding complaints, second surgical intervention was performed under general anesthesia. There was a solid mass in the prostatic urethra (Fig. 1). The mass and adenomatous tissue in the prostatic urethra were resected. The histopathological examination of the mass revealed malignant fibrous histiocytoma. The histopathological examination of the resected adenomatoid tissue revealed benign prostatic hyperplasia. Following diagnosis, chest and upper and lower abdominal computerised tomography studies showed no metastasis. Bone scintigraphy findings were normal. Histologically, malignant fibrous histiocytoma (MFH) consisted of spindly fibroblasts with large numbers of bizarre, multi-nucleated giant cells. There was a tendency of some of the mononuclear cells to resemble histiocytes. The cells were typically arranged in a “storiform” or “carriage wheel” pattern radiating out like curved spokes from a central point (Fig. 2). Immunohistochemical stains on the original tumor were positive for CD68 and vimentin. Stains for muscle differentiation (desmin and muscle-specific actin), melanocytic differentiation (S-100 protein), PSA and epithelial differentiation (low molecular weight cytokeratin) were all negative. DISCUSSION Malignant fibrous histiocytoma is the most common adult soft tissue sarcoma, comprising 10% to 21% of all such tumors (1, 2). Primary involvement of the genitourinary tract is extraordinarily rare. The most common site is the kidney and the least is prostate (4). In literature review we could find 7 cases (3, 5-10). Clinically and radiologically MFH of the prostate cannot be differentiated from other prostate neoplasms .On physical examination patients are found to have a diffusely enlarged and firm prostate (3). In our case the prostate was small and the mass was seen in the urethra. Approximately 50% of patients have a history of typical aciner adenocarcinoma of the prostate (9). Almost 25% of the patients have metastases at the time of diagnosis (9). Metastases from MFH usually involve lungs and lymph nodes (3). No parameter, including age, history of radiation or androgen deprivation therapy, histological subtype, percentage of necrosis, percentage of sarcoma, sarcoma grade, or Gleason grade of the adenocarcinoma, was found to be predictive of outcome (2, 6, 9, 10). Factors predictive of long-term survival were negative surgical margins and absence of metastatic disease at presentation (3, 9, 10). Serum PSA concentrations at the time of the diagnosis of carcinosarcoma suggests that this assay is not valuable in early detection of tumor. Similar results have been reported for serum prostatic acid phosphatase (9, 11-13). The role of antiandrogen therapy and radiotherapy in the treatment of prostate carcinosarcoma is questionable (9). Malignant fibrous histiocytoma is only moderately sensitive to radiotherapy and chemotherapy and the advocated treatment is extensive surgical excision (2). The outcome of MFH is generally very poor with a recurrence rate after removal of tumour of more than 50%. A 4 year survival of less than 14% (2, 14). In conclusion MFH is seen very rarely in urinary system especially in prostate. Probability of development of MFH after prostate adenocarcinoma should be kept in mind. REFERENCES
Copyright 2008 - Medical Investigations Society The following images related to this document are available:Photo images[gm08025f2.jpg] [gm08025f1.jpg] |
| |||||||||

{kind=link}
{kind=link}