 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
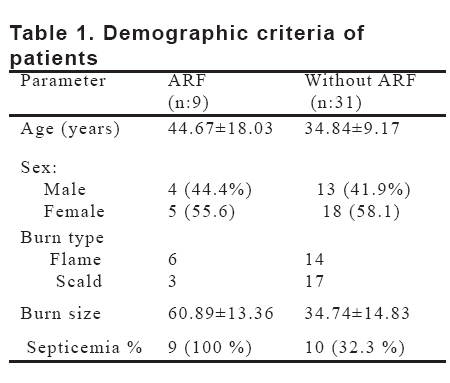
European Journal of General Medicine, Vol. 5, No. 3, 2008, pp. 126-133 Markers Of Tubular And Glomerular Injury In Predicting Renal Outcome In Thermal Burn Patients Alaa Sabry1, Ahmed Bahaa El-din2, Al Moddather El- Hadidy2, Mohammed Hassan2 Mansoura University, Medical Faculty, Mansoura Urology and Nephrology Center, Departments of Nephrology1 and Plastic surgery2, Egypt Code Number: gm08026 Aim: Thermal injury elicits several systemic consequences. Acute renal failure (ARF) is a well known complication of severe burn and is an important factor leading to an increase in mortality. We aimed to focus on early diagnosis of acute renal failure occurring in major burns and to determine the predictors for acute renal failure.
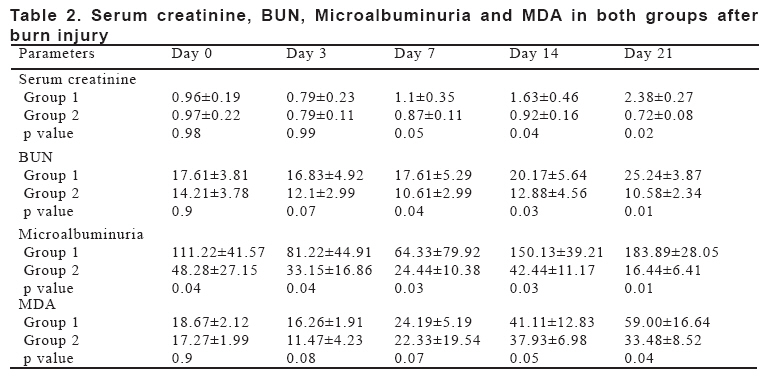
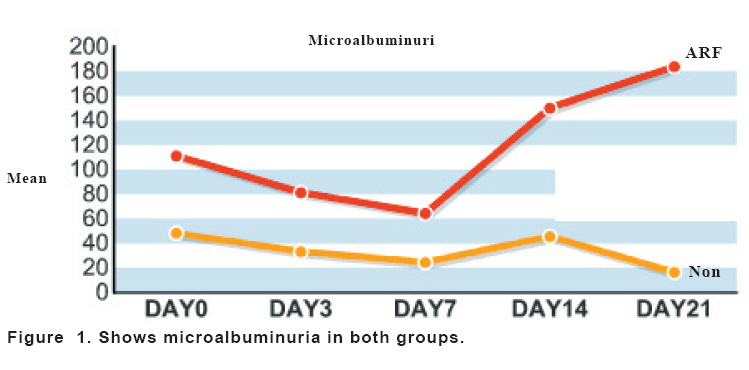
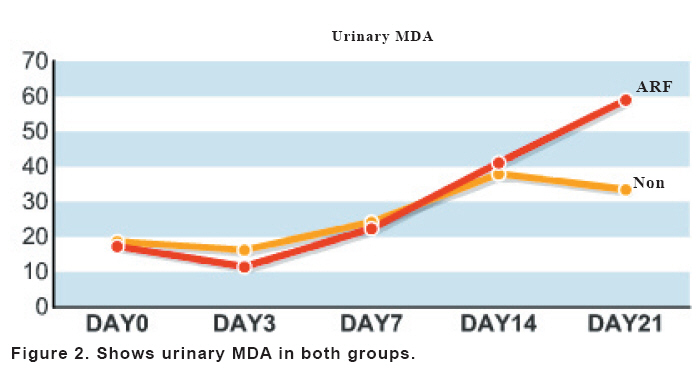
Key words: Acute renal failure-thermal- Burn. INTRODUCTION With recent advances in the systemic care of burn, understanding the pathophysiology of severe burn injury and systemic inflammatory response syndrome, patients with burn covering up to 80% of their body surface area can frequently survive (1). Burn is not only skin injury but serious systemic illness often accompanied by various complications. Multi-organ injury complicating severe burn constitute up to 50% of mortality cases (2). Acute renal failure (ARF) - that complicates 13-38% of burned patients admitted to hospitals - is a well known major complication of severe burn carrying an extremely high mortality (3). Several variables are considered as important predictors of ARF in burn patients, occurrence of septicemia, fluid loss, muscle damage, hypotension and cardiopulmonary failure as well as the use of nephrotoxic agents are among these factors (4). The onset of ARF- whether early (less than one week) or late- with delay of energetic and intensive management of burn lesion- carry a significant impact on the development of ARF as well as on enhanced mortality from uremia (5). The major etiologic factors in the early development of early ARF after burns are hypovolemia and decrease in cardiac output. The resultant decrease in renal blood flow is primarily responsible for the oliguria seen immediately after burns, while filtration failure and tubular dysfunction are caused by various factors and interacting with each other (6). Renal insults in burns are characterized by the development of extensive inflammation inducing an intensive acute phase response in the kidney. Burn injury initiates significant oxidative stress that induces ARF as well as multi-organ failure (7). Serum creatinine, creatinine clearance, urinary protein excretion, microalbuminuria and urinary malondialdehyde (MDA) are used to assess the incidence of both glomerular and tubular dysfunction and as index in treating ARF in burned patients. In view of these findings we decided to evaluate the incidence of ARF in thermal burn patients, to evaluate various prognostic and predictive factors involved in the pathogenesis of ARF in burn patients in addition to evaluation of early therapeutic interventions. Also we investigated the influence of burn size and the presence of septic manifestation on the occurrence of ARF in patients with major burns. MATERIALS AND METHODS Forty patients with moderate to severe thermal burn injury - second and third degree burns covering 20 to 70% of their body surface area (BSA) - constituted the material of our study. They were admitted to Mansoura Emergency Hospital within 24 hours of their injury. They consisted of 17 males and 23 females, their age ranged from 9 to 70 years. This protocol met the requirement of local ethical committee and all patients consented prior to the study. Resuscitation All patients were resuscitated with crystalloids followed by colloids according to the Parkland formula (4 ml/kg/%BSA/first 24 hours); colloids were given as albumin, fresh frozen plasma during the next 24 hours. The infusion volume was adjusted to produce a mean hourly urine output of 50 ml/h during the first 24 hours and 100 ml/h during the second 24 hours after insertion of Foley catheter. The burn wounds were thoroughly and gently cleaned by immersing the patients in a whirlpool bath to which sodium hypochlorite had been added (150:1). The wounds were then debrided by a surgical sponge, rinsed, dried and 1% silver sulfadiazine cream was applied and then covered with dry coarse mesh gauze, this procedure was done daily inpatients. Surgical treatment included early excision and grafting with autografts as indicated. Catecholamine was administered when appropriate to maintain sufficient hemodynamic stability. Antibiotic was given according to the patients need and culture with exclusion of nephrotoxic drugs. Nutritional support The goal of nutritional support was to maintain a positive nitrogen balance by greater than 6 g/day. Exclusion criteria Those with previous renal dysfunction, diabetics, hypertensives and pregnant ladies were excluded from our study. All patients were subjected to routine investigations where arterial blood gases done twice daily, complete blood count, liver function, blood culture, coagulation profile, plain chest X-ray were done every week. Assessment of renal function Urinalysis, serum creatinine, blood urea nitrogen (BUN), fractional excretion of sodium, urinary Malondialdehyde (MDA) and microalbuminuria was done on day 0, 3, 7, 14 and 21. All samples were analyzed in duplicate. Urinary Malondialdehyde MDA was isolated and quantified according to Guichardant et al., 1994 (8) on SPEKOLL 11 using the following equation: Test/standard x concentration of test. Urinary microalbuminuria was defined by albumin excretion rate between (30-300 mg/day) determined by radioimmunoassay using (Org SMA Immunoassay procedure kit- Orgenetic Diagnostika GmbH, Mainz). Fractional excretion of Sodium (FENa): Was calculated according to the following formula: FENa= UNa X PCr X 100 PNa X UCr Where UNa= urinary sodium, UCr = Urinary creatinine PNa= Plasma sodium, PCr = Plasma creatinine A value below one precent suggests prerenal ARF, a value between 1-2 may be seen with either disorder, while a value above 2 percent usually indicates oliguric ARF. Renal replacement therapy It was initiated at a serum creatinine level > 4 mg% (with rising tendency) combined with a blood urea nitrogen level >200 mg/dl or in patients with anuria or oliguria (urine volume < 400 ml/24 hour) with anasarca and/or hyperkalemia. Statistical analysis Was performed using the SPSS for windows software package release 11. Data are presented as mean and standard deviation. Student T-test and chi-square-test were applied as appropriate. Stepwise multiple regression analysis of data was carried out to predict most relevant variable affecting the development of ARF. A p value of ≤ 0 .05 was considered significant. RESULTS A total number of 40 patients-who met our inclusion criteria - were admitted to the burn unit presenting with second and /or third degree burn (more than 20% of total body surface area) during the period from May to December 2005 constituted our study group. Demographic parameters are presented in Table 1. There were 17 men and 23 women with a mean age of 44.67±18.03 years for those who developed ARF and 34.84±9.17 for those who did not develop ARF. The burn type was flame burn in 50% of patients and scald burn in the other half of patients. None of the patients had evidence of chronic renal failure, diabetes, hypertension, or were pregnant. Incidence of renal failure Nine patients (22.5% of all cases) developed ARF (defined by rising of serum creatinine > 2 mg/dl and blood urea nitrogen (BUN) > 25 mg/dl) during the 3rd week with the onset of septicemia. These were gradually increased from day 7 postburn until the end of second week reaching maximum level at the third week after burn (Table 2). Four patients required supportive dialysis as their serum creatinine exceeds 4 mg %. Patients who did not develop ARF were early resuscitated from the start and received all supporting measures that maintain the renal function and improve hemodynamic parameters. Their serum creatinine and BUN levels were within normal levels at different time intervals of the study (Table 2).Univariate analysis study of data has shown no impact of burn type, age, sex on incidence of ARF following burn. Markers of renal damage Microalbuminuria The group that developed ARF showed microalbuminuria starting from day 0 reaching up to 3 or 4 fold its normal on day 14 and up to a maximum level on day 21. This pattern was consistent with elevations of serum creatinine and BUN. Microalbuminuria progressed to overt proteinuria in 3 cases (Figure 1). Urinary MDA Urinary MDA was elevated before developing ARF in the group of patients who developed ARF about 3 folds their normal values. It was gradually increased on day 14 reaching maximal level on day 21 (Figure 2). Fractional excretion of Na In all cases that developed acute renal failure FENa was above 2% indicating ATN. Incidence of septicemia In this study, “sepsis” was defined as a blood culture revealing the pathogen during the hospital stay or at autopsy. All patients who developed ARF have experienced septicemia during the 3rd week – proven clinically and by bacterial culture - in contrast to only 10 patients among those who did not develop ARF . Microbiological analysis revealed that Staph aureus in 14 patients, pseudomonas aeroginosa in 6 patients , Klebsiella species in 4 patients , Acinetobacter in 2 patients, Streptococcus in 2 patients and Candida albicans in one patien respectively. Mortality 2 cases (22.2%) in ARF group died on days 32nd and 36th after burn. Both cases were septicemic and required dialysis support. Predictors of ARF Burn size % and occurrence of septicemia were the only predictors of ARF in burn patients by multiple regression analysis (SE B 0.003 and 0.104- P value 0.001 and .0371 respectively). DISCUSSION Although ARF was reported to complicate 13-38% of the admissions of burned patients, this complication merits a special attention in that its outcome is generally very poor and varies depending on the severity and adequacy management of the burn injury. Burns are one of the most serious of all pathologies with regard to the surgical and intensive care aspect of treatment. Unlike other surgical pathologies, it requires initial intensive care for two to three days a period which coincide with treatment of burn shock. In prolonged courses of pathology there may be disequilibrium of all physiological indices (hydroelectric and acid base balance, hematological condition and nutrition). Failure to correct these in due time may subsequently aggravate the general prognosis and pave the way for complication. Extensive cutaneous burn produces local changes which may cause general effects involving every system of the body (3). The incidence of ARF in our study was 22.5% which is relatively higher than what is reported in other studies (9,10). However the incidence of ARF after thermal injuries appears variable according to what has been reported in the literature (4). This could be explained by the fact that it depends on the severity of the burns and on the definition of ARF which is different from one study to another. The higher burn size in our study- (≥ 61%) which is considered as very severe burn- could also partially contribute to the high incidence of ARF. In agreement with our results, Holm et al. (4) reported an incidence of ARF (14.6%) in his series in 328 patients with burns > 10%. Two different presentations of ARF have been recognized in burned patients. ARF that occurs immediately after burns is generally thought to be due to a decrease in renal perfusion resulting from hypovolemia which is related to extensive fluid losses from the burn wound, a fluid shift from the circulation into the interstitial or intracellular space, or a delay in fluid resuscitation which can accentuate the low volume circulation. The decrease in renal blood flow with inadequate resuscitation causes oliguria (6). Furthermore, it has been shown that burn stress and its associated circulatory derangement stimulate the release of stress-related hormones, such as catecholamine, angiotensin II, aldosterone, and vasopressin (6-10). These hormonal changes cause vasoconstriction and changes in regional blood flow, particularly in the kidneys (11). On the other hand the later appearance of acute renal failure is mainly associated with systemic sepsis, and is usually accompanied by other organ failure such as pulmonary insufficiency, liver failure, or disseminated intravascular coagulopathy (11). This is a period that is associated with an increase in serum levels of cytokines (tumor necrosis factor, interleukin 1, etc), eicosanoids (prostaglandins, thromboxane and leukotrienes), Elevated levels of stress-related hormones also cause vasoconstriction, fluid retention and renal hypoperfusion with tubular necrosis leading to acute renal failure (6-12). The administration of nephrotoxic antibiotics, such as aminoglycosides and certain cephalosporins that are often used in treating burn infections is also a factor that may cause acute renal failure (13). The vasodilator prostaglandin E2 is found in the kidneys and counteracts the effect of many vasoconstrictors. Its production, however, is inhibited in the early phase of burns and when sepsis develops (6,11,13). Other circulating mediators that originate from the burn wound such as IL-6, IL-8, and tumor necrosis factor, contribute to the hypermetabolic and inflammatory response in burned patients (14). Although these mediators were not examined in our study, we can not deny their role. The objective of laboratory examinations in severe burns is to assess markers of ARF which helps early diagnosis, management and treatment of ARF aiming to decrease mortality. Fractional excretion of sodium (FENa) is an accurate screening to differentiate between prerenal ARF and acute tubular necrosis (ATN) which are the commonest causes of ARF in burn patients. We found FENa more than 2% in those patients who developed ARF indicating ATN due to dehyderation and or septicemia. Increased urinary excretion of protein is one of the most common and easily detected signs of renal pathology. Renal abnormalities may occur both in the quantity and in the composition of urinary proteins (15). Microalbuminuria is still regarded as one of the most sensitive markers that reflect glomerluar injury (16). In our study microalbuminuria was maximal on the day of admission and decreased gradually thereafter in patients that did not develop ARF with improvement of their hemodynamics and good resuscitation while there was a constant rise in patients developing ARF after the second week with development of infection and septicemia . These results are in concordance to what reported by Kang HK et al (17). This is also supported by data from animal and clinical studies demonstrating that burn shock manifests lesions in the renal tubules and glomeruli with high and low-molecular weight proteins appearing in the urine (6-12). It is known that burn injury initiates an appreciable oxidative stress and inflammation leading to severe multiple organ failure (7). Free radical production is associated with inflammation and circulating lipid peroxides have been shown to increase in burn patients during the first week post injury (18). Oxidants are major products of inflammation and lipids peroxides have been shown to increase in the plasma of burn animals and patients (7,19). The end products of lipid peroxidation include aldehydes and hydrocarbon gases. The most commonly measured product is MDA which is known to react with proteins and amino acids (20). Urinary MDA is a gross indicator of enhanced lipid peroxidation in renal tubules and directly proportional to renal damage (21). A close relationship between the intensity of lipid peroxidation and complications after burns has been reported (22). In our study 24 hour urinary excretion of MDA was increased in all cases that developed ARF reaching up to 3-5 folds its value before rising of serum creatinine and BUN and continuously increased thereafter while in the rest of cases that did not develop renal failure there was gradual decrease after controlling of infection and improving body hemodynamics confirming that lipid peroxidation is strongly activated after burns. We can suggest that renal inflammation and tubular injury in burned patients persist during the 3 weeks after the burn injury in spite of early and aggressive management. These results are in agreement with what reported in earlier studies (15,17). This pattern of changes in the urinary MDA appears to be a very sensitive biochemical parameter and may be a useful in assessment of renal status (8-17). Sepsis has been identified as a major factor contributing to mortality in burned children with acute renal failure (23). Recently it has become accepted that early fluid resuscitation and the prevention of sepsis may reduce the incidence of acute renal dysfunction in burned adult victims (24). In our study sepsis was diagnosed in all cases that developed ARF compared to 30% in cases with normal renal function. These results appear to coincide with that reported by Brive et al. (25). However this incidence of septicemia is higher than that is reported by Marc G. Jeschke et al. (26)1% incidence of sepsis in patients with ARF- and Charlotte Holm (4) who reported an incidence of sepsis of 91% of patients with late ARF. The explanation behind this may be due to different degrees of burn size in our and their patients. As an effort to find etiological factors for the development of ARF we compared patients without renal insufficiency with patients developing ARF using multiple regression analysis, it was clear that burn size is highly significant independent risk factor . Patients with ARF had mean burned surface area of 61% signifying that wide surface area predispose to excessive loss of extracellular fluid and albumin , as well as providing good chance of increase of infection hazards. Only burned body surface area proved to be significantly correlated with the development of ARF, whereas age, third degree burn or electric injury was not significant. This is in accordance with the findings of previous authors (1,2,27). In addition to surface area burned, the second predictive factor for developing ARF was the presence of severe septic complication and significantly correlated with the development of ARF. This is in accordance with the finding of previous authors (9-28). It is well known that with the onset of renal insufficiency the prognosis of the burn patient becomes remarkably unfavorable, as most studies have reported a mortality rate of around 80%.This may be due to the fact that the pathophysiology of ARF in burned patients is poorly understood; we still do not know why renal failure develops in these patients and what we can do to prevent its occurrence. However there is a trend toward a lower mortality in burned patients with ARF in recent years (29). In our study the mortality rate in patients with ARF was 22.9% and death was due to multiple organ failure in these 2 cases. However, no firm conclusion can be drawn because of the small number of patients. Interestingly, survivors almost uniformly recover a normal renal function. In conclusion ARF was found to complicate 22.5 % of burn patients and was found to be related to the size and depth of burn. Development of septicemia after burn can trigger a series of inflammatory reactions and mediators that lead to multiple organ dysfunctions including renal damage. Early detection of ARF should be carried out by assessment of renal function (both glomerular and tubular function) that should start from the day of admission. Microalbuminuria and urinary MDA are good markers for prediction of ARF in burn patients. Minimizing renal damage in burn depends on integrated effort of early and rapid resuscitation and early diagnosis of renal affection . REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08026f2.jpg] [gm08026t1.jpg] [gm08026f1.jpg] [gm08026t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}