 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 3, 2008, pp. 134-139 Study Of The CLPTM1 Gene In South American Non-syndromic Cleft Lip Patients With Or Without Palate Mehmet A Sözen1,3, Marie M Tolarova2, Richard A Spritz3 Afyon Kocatepe University, Medical Faculty, Department of Medical Biology1, Afyonkarahisar, Turkey, University of the Pacific, Department of Orthodontics2, San Francisco, University of Colorado Denver, Human Medical Genetics Program3, Aurora, USA Code Number: gm08027 Aim: The CLPTM1 gene is considered as a candidate gene based on the fact that it is localized in the human chromosomal region 19q13 which maps in the candidate region OFC3. This study aims to test the involvement of this candidate gene, CLPTM1, in non-syndromic cleft lip with or without cleft palate (CL/P, MIM 119530) and to analyze particularly a CLPTM1 variant, A88A if there is an allelic association with non-syndromic cleft lip and palate.
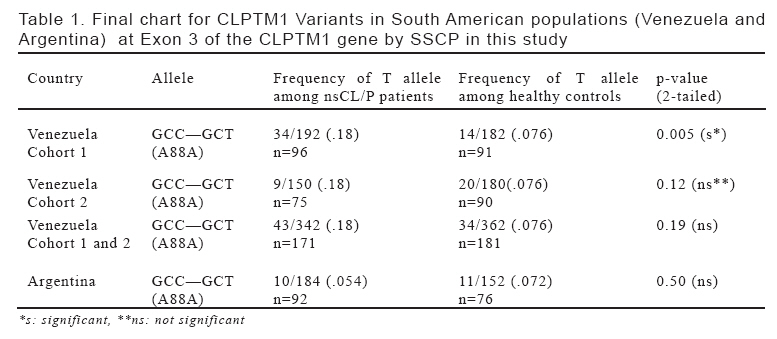
Key words: CLPTM1, human chromosome 19q13 region, cleft lip/palate, mutation, SSCP INTRODUCTION Cleft lip with/without palate (CL/P) is is perhaps the most common major birth defect and occurs in approximately 0.4-2 per 1000 liveborn infants in most populations depending on the geographic origin and ethnic background worldwide (1,2) In man, about 30% of cases are syndromic and in the rest (70%) of them, CL/P occurs as an isolated, sporadic defect where the clefts are without other anomalies. Such ‘non-syndromic’ CL/P (nsCL/P, MIM 119530) is a polygenic, multifactorial disorder, showing complex inheritance and thought that both genes and environmental factors, contributing either independently or in combination, are responsible for that kind of clefting (3-7). Recently, considerable evidence suggested that a gene on chromosome 19 q1.31-2 region could play a role in non-syndromic cleft lip with or without cleft palate by linkage analyses (8-11) and association studies (12,13) performed in different populations. As a result many candidate genes as well as microsatellite markers were analyzed to test their involvement in non-syndromic cleft lip with or without palate (14,15). In this region, chromosome 19q13, some of the candidate genes tested for the involvement in the nsCL/P formation were BCL3, PVR, PVRL2 and CLPTM1and the studies are focused on mainly these four candidate genes. First, BCL3 has been considered as the most prominent candidate gene (8,16) and has been suggested to play a role in nsCL/P. Recently PVR and PVRL2 has been also added to the list due to two reasons: 1. To be localized in the chromosome 19q13.2 and an allelic association was found (17) though it was not supported by another report (18) as well as belonging to the same nectins gene family (19,20) of which one member (PVRL1) in particular is shown to play a role in both a syndromic and non-syndromic versions of cleft lip/palate (21,22). CLPTM1 gene is tought to be another candidate based on the observation of a translocation occured in a family with cleft lip palate (23). It was originally identified in a family in which cleft lip and palate segregated in two of three generations with a balanced chromosomal translocation t(2;19)(q11.2;q13.3). It is also localized in the same chr19q13 region and implicated in aetiology of the nsCL/P as a genetic component. Recently in another report, Turhani et al., have also analyzed the sequence changes in CLPTM1 gene together with PVRL1 variations in nsCL/P patients versus controls and reported no sequence changes in exons 4,5,7,9,11,12 and 14 in any of the patients and the controls, however, they reported some intronic changes in the following introns: two changes in IVS13 and IVS2, one in IVS3, IVS6 and IVS7 as well as several synonomous changes two of which are in exon 8 (Pro309Pro and Gly331Gly) and one in exon 3 (Ala88Ala). Also they reported that a PVRL1 variant, Glu441-Gly442 ins Glu, was found more frequently in the nsCL/P patients and none of the controls (24). However, they suggested that simultaneous occurrence of an intron change, exon changes of the CLPTM1 gene and Glu441-Gly442 ins Glu mutation of PVRL1 could be a genetic factor for non-syndromic clefts. They also emphasized the importance of investigation with more patients and controls in a manner of multi-centre studies. In another study by both population- and family-based analyses, no positive association was found between CLPTM1 and nonsyndromic CL/P in the Japanese population (25). The CLPTM1 gene was also studied to test its role in human cancer (26) as well as in gene expression in reproductive organs and to identify genes that play a crucial function in sexual reproduction in a plant (27). We have previously shown that homozygous PVRL1 mutations result in a rare autosomal recessive CL/P syndrome, termed CLPED1, (21) whereas a heterozygous nonsense mutation of PVRL1 is associated with sporadic nsCL/P in northern Venezuelan patients (22). The aim of this study was to examine the entire sequence of exon 3 of the CLPTM1 gene in order to determine whether or not variants of the CLPTM1 gene, especially the synonymous mutation A88A, participate in CL/P development in the Venezuelan and Argentinian populations. For this, a mutation screening for exon 3 of CLPTM1 gene were attempted followed by the calculation of the allele frequencies and then an allelic association between the synonymous mutation A88A of the CLPTM1 gene and non-syndromic cleft lip with or without palate malformation was tested in the Venezuelan, and Argentinian populations. MATERIALS AND METHODS Subjects Bloodspot samples to be used for genomic DNA isolation were obtained with informed consent from patients with nsCL/P, and population-matched controls from two different populations from Venezuela, and Argentina in South America. We sampled 96 nsCL/P patients and 91 controls for cohort 1 (Grid 1) and 75 nsCL/P patients and 90 controls for cohort 2 (Grid 2) constituting a total of 171 nsCL/P patients and 181 controls from northern Venezuela. We also sampled a total of 92 nsCL/P patients and 76 controls from another South American country, Argentina. Polymerase chain reaction, mutation screening, genotyping and statistics We screened the exon 3 of CLPTM1 gene including the adjacent intron and non-coding sequences, by simultaneous SSCP/heteroduplex analysis for south and central American samples. The bloodspots were used to isolate genomic DNAs (28) and then these genomic DNAs were used as template for polymerase chain reaction (PCR) using the following primers: 5’-CTAAGTCAGAAGGAAGTCAG-3’ (forward primer) and 5’-CATCACTCCTCCACATTCCA-3’ (reverse primer). PCR reactions were done in accordance with the Commpany’s instructions (Ýnvitrogene) using Platinum Taq DNA polymerase and accompanying buffers in a 10ul reaction volume. Variants were determined by electrophoresing the amplified products in 0.5X MDE gels (Biowhittaker Molecular Applications) containing 10% glycerol (29). PCR products showing novel aberrant SSCP/Heteroduplex patterns were subjected to standard DNA sequence analysis. Statistical analyses of allele frequencies were carried out using Fisher’s exact test and 2-tailed P-values were calculated. RESULTS We first carried out a mutation analysis for exon 3 of CLPTM1 gene among 96 unrelated patients versus 91 unrelated South American controls from northern Venezuela for cohort 1. We screened the entire sequence of exon 3 of the CLPTM1 gene, and adjacent intron and non-coding sequences, by simultaneous SSCP/heteroduplex analysis for South American samples, followed by DNA sequencing of PCR products that contained apparent variants. Consequently, we determined a synonymous change (CT resulting in a silent change, A88A) which was already reported by Turhani et al. (24) and was particularly common in both patients and controls. And then we calculated mutant T allele frequencies for this synonymous change and tested for the presence of statistical significance using Fisher’s exact test. As shown in Table 1, as a result comparing simple allele frequencies for the A88A synonymous change in nsCL/P patients versus controls within Venezuelan population, we observed significant difference in allele frequencies between patients versus controls for cohort 1 showing an elevated T allele frequency in patients (p=0.005). Afterwards, for the same A88A change we decided to extend the test for another cohort (Grid 2) from Venezuela to confirm the finding and the significance of this T allele (Table 1). For this, we genotyped another cohort (Grid 2) including 75 cases and 90 controls from the same region (Cumana region in Venezuela). In contrast to the finding obtained from the first cohort (Grid 1), this time we found lower frequency of the T allele in patients. When the data from the two grids were combined; though the overall frequency of the mutant (T) allele was still slightly elevated in the patients, however, the significance has disappeared. As a result there was no significant difference in terms of T allele frequency for the variant in question (P88P) among the cases versus controls. And this led to the significance has gone off. Overall, we concluded that there was no association between particularly a CLPTM1 variant (A88A) and non-syndromic cleft lip with/without palate (nsCL/P) malformation in Venezuela. Then we also screened the same synonymous change (A88A) of CLPTM1 gene in nsCL/P patients versus controls from another South American country, Argentina, to investigate the case conflicting in the two cohorts of Venezuela (Table 1). We observed no significant difference between nsCL/P patients versus controls in Argentina. This confirms the previous results obtained from South American (Venezuela) population showing the lack of association between particularly a CLPTM1 variant, A88A, and nsCL/P also in Argentina. During this screening for the exon 3 synonymous change, we found another two rare synonomous variants in the exon 3 of CLPTM1 gene in Venezuelan population. One was a synonymous change (P85P) detected only in two patients and none of the controls. However, it did not also differed between nsCL/P cases versus controls. The other was found as an intronic change in the (IVS3+37 T/G) affecting 9 patients and 3 controls as a heterozygous form whose frequency was observed slightly higher among CL/P patients than the ones among controls, though not significant (p= 0.12). DISCUSSION Non-syndromic cleft lip with or without palate (nsCL/P) is a complex disorder and its aetiology is still largely unknown. So many genetic and environmental factors possibly seems to be contributing to the development ns CL/P. So far linkage analysis and associations studies suggested that several chromosomal regions including chromosome 19q13 and several candidate genes might be involved in the aetiology of the non-syndromic clefting malformation (11,12,15,16,17). CLPTM1 was also considered as a candidate gene which was initially identified at translocation break-point segregated 2-3 generation in a family with cleft lip and palate and it is localized at chromosome 19q13 (23). In another report by Turhani et al., it was screened for associated mutations with non-syndromic cleft lip with/without palate and they suggested that simultaneous occurance of CLPTM1 variations with a PVRL1 variant in the patients with non-syndromic cleft lip with/without palate could be a genetic risk factor, though the sample size were relatively small (24). However no other supportive reports in larger populations appeared lately. In the present report, however, we carried out a case-control survey particularly for a synonymous variant of exon 3 of the CLPTM1 gene to test its involvement in the formation of nsCL/P malformation. However, our data does not seem to support a role for the CLPTM1 exon 3 variant in the aetiology of the nsCL/P. These data also suggest that sample size for allelic association studies is very important based on the allele frequencies of A88A observed. The other two CLPTM1 variants, IVS3+37 T>G and P85P, observed in the course of the study might be normal rare polymorphisms seen in the population studied. In addition, regarding single stranded conformation polymorphism (SSCP) technique, it is not possible to detect all variants being present in patients, and some variants that might contribute to nsCL/P are likely to be missed. Moreover, we cannot exclude the possibility of other variations might exist in non-screened sequences and also might include regulator elements either in the intronic regions or upstream and downstream of the gene. These undetected variations are likely to affect the expression of the gene to some extent. Therefore, it suggests further analysis of the other exons and the upstream promoter region potentially including regulatory sequences of the gene might give better picture if CLPTM1 is involved in the development of nsCL/P malformation. This remains to be elucidated in the future. In conclusion, no significant difference was observed in the number of patients versus controls particularly for the CLPTM1 exon 3 variant A88A. Thus, these results does not support a role for CLPTM1 variants (A88A in particular) to participate in the formation of nsCL/P in the populations studied. However, we can not rule out the possibility of undetected mutations either due to the restrictions by SSCP technique used or possible mutations in other intronic, and upstream or downstream regions of this gene potentially containing the regulatory elements which is not analyzed in this study. More works are needed to be done in different populations to support the role of CLPTM1 gene variations in the formation of nsCLP malformation as well as a genetic risk factor in the formation of the nsCL/P. ACKNOWLEDGMENTS This work was supported by grant DE13571 from the National Institutes of Health (R.A.S.) and by support from Rotaplast International, Inc. (M.M.T.). REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08027t1.jpg] |
| |||||||||

{kind=link}