 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 3, 2008, pp. 147-151 The Measurements Of Intervertebral Foraminal Area And Angulation Of Cervical Vertebra Before And After Anterior Cervical Discectomy Murat Coşar1, Mehdi Sasani2, Faik Sungurlu3, Ali Fahir Özer2, A Celal İplikcioğlu4, Ali Çetin Sarıoğlu2 1Kocatepe University, Faculty of Medicine, Department of Neurosurgery, Afyon, 2 VKV American Hospital, Department of Neurosurgery, 3 Haydarpasa Numune Education Hospital, Department of Radiology, 4 Okmeydani Education Hospital, Department of Neurosurgery, Istanbul, Turkey Code Number: gm08029 Aim: There are two main problems after cervical discectomy without using bone graft or methalic instruments; angulation and foraminal stenosis. We evaluated these problems which occur after cervical discectomy.
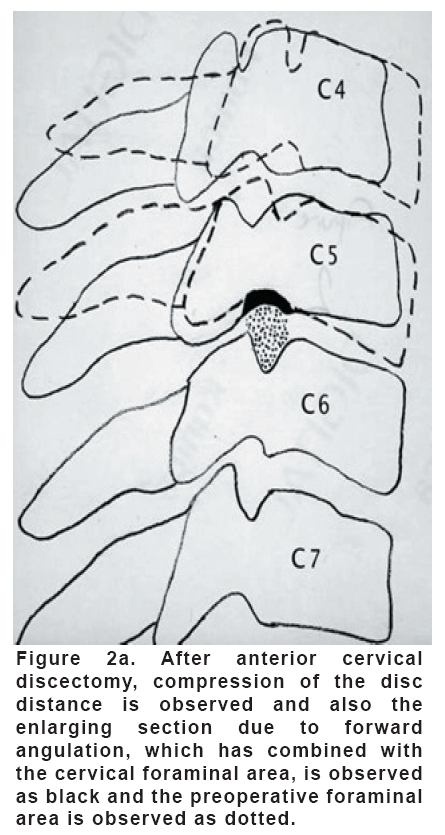
Key words: Angulation, anterior cervical discectomy, intervertebral foraminal area INTRODUCTION Cervical radiculopathy may be caused by an herniated nucleus pulposus or osteofit formations. Although anterior or posterior surgical procedures are performed for cervical radiculopathy, their effects on cervical intervertebral foramina are still being discussed. Recently, anterior cervical approaches are much prefered. After the anterior cervical discectomy, there are some surgical procedures where autograft, allograft or carbon cages are placed into the intervertebral disc space (1). In this study, we viewed the control MRI of 13 cases who had been operated via anterior cervical discectomy. We measured the right and left side foraminal areas in the sagittal sections of MRI and studied how the foraminal areas were affected from the postoperative angulation of the cervical vertebra. MATERIAL AND METHODS We studied on 13 patients (8 female, 5 male) whom were performed simple anterior cervical disc hernia operation. The average age of the patients was 48.6 (between the ages 35-58). The operation levels of patients were; one at C4-5 level, ten at C5-6 level and two at C6-7 level. All of the patients had taken their follow-up MRI at the same radiology center regarding the fact that one year had passed since their operations. Additionally, the sagittal sections of MRI showing the right and left intervertebral foramina were chosen for measurements. Totally, 26 intervertebral foramina were studied in 13 patients. The sagittal MRI of all patients before and after their operations, were scanned, thus making it possible for them to be viewed and studied on computer. The intervertebral foraminal areas of these images which had been transferred to computer were calculated in terms of milimeter square by the help of a computer program (Imagej version 1.33i, Medientehnik und Design, Hagenberg, Austria, 2004). Measurement results of preoperative and postoperative foraminal areas on the right and left side of the discectomy level were compared with statistical methods. The sagittal images passing from the midway of the vertebra corpuses were taken as the basis to measure the angulation. Taking the discectomy level as basis point, linear lines were drawn in such a way that these lines pass from the posterior of the vertebra corpuses which stand 2 up and 2 below of the discectomy level; thus an angle is formed and then the angulation was measured in preoperative and postoperative sagittal MRI sections. The clinical condition of these patients and their pain scoring were compared by using the Copenhagen Neck Disability Scale (CNDS) before and after the operation. We asked 15 questions to the patients about their neck disability and evaluated each answer with 2 the base of points. Additionally, we asked to the patients if they have radicular symptoms or not. RESULTS These 13 patients were evaluated under two groups. Eight of the patients had no forward angulation (patients 1-8) and 5 of them had forward angulation (patients 9-13). It has been observed that the patients who have no appearant changes in their cervical angulations or the ones who preserved their status (Figure 1a, 1b and c), their right and left side measurements showed significant decrease (p≤0.05) in the foraminal areas; whereas the patients with increasing cervical forward angulation by 100 degrees or more (Figure 2a, 2b and c), right and left side measurements revealed a significant increase (p≤0.05) in their intervertebral foraminal areas. CNDS showed that all of the patients in both groups have significant difference when compared the preoperative and postoperative symptoms (p≤0.05). The radicular symptoms of both groups are also decreased. DISCUSSION Intervertebral foramen is an ovoid shaped bone structure through which the spinal roots pass and the up and down notches of the vertebrae form its base and top (2). Due to a decrease in intervertebral disc space, a decrease can also be seen in the intervertebral foraminal dimensions (3,4). It has been observed that 82 % of the patients with degenerative spondylosis, showed decrease in the intervertebral foramina in their radiological views due to the reduction of the intervertebral disc space (5). After a cervical discectomy operation, reduction in the intervertebral foraminal dimensions might occur and compression of the spinal roots might be observed due to the reduction in the intervertebral disc space (3,4,6,7). Intervertebral foraminal dimensions are vital for radiculopathy and foraminal stenosis diagnosis. Foraminal stenosis is a dynamic condition because it affects the diameter of the intervertebral foramina during the flexion and extention of the vertebra (3,8-10). During their research, Moyoux-Benhamou et al. (11) had observed that the intervertebral foraminal height reduces with a percent of 18 while the cervical vertebra passes from flexion condition to full extention condition. Farmer and Wisneski (8) observed a significant increase in pressure on C5, C6 and C7 spinal roots during extention condition and also they informed that this pressure increase on spinal roots, disappears during neutral status. In another similar study, Lu et al. (3) informed that in cases where the intervertebral disc space reduces, the intervertebral foraminal area also reduces. In our study, we observed that in cases, where the intervertebral disc space had collapsed after operation and where there was no appearance of forward angulation (Figure 1a, 1b and c), the measurements of right and left side foramina revealed significant decrease (p≤0.05) as we had already been informed by the results of previous studies. In addition to this, we observed that in the cases having 100 degrees or more forward angulation after the operation (Figure 2a, 2b and c), the intervertebral foraminal areas enlarge up to a significant extent due to distraction that has developed on the back spinal colon. When compared with the preoperative neurological examinations, significant progresses have been observed in all the patients during their postoperative neurological examinations and also significant progresses have been observed when comparison was made by using CNDS for preoperative and postoperative periods (p≤ 0.05). But; the patients who had anterior cervical discectomy operation and whose intervertebral foramina enlarged by making a forward angulation, showed significant progresses in their neurological status after the operation (p≤0.05). In all these cases, muscular tension type headaches were observed. The patients who had anterior cervical discectomy operation and whose intervertebral foraminal area had decreased due to the collapse of intervertebral disc space showed radicular irritation symptoms. None of these patients had been reoperated. As it is well known, the cases in which there is forward angulation, muscular tension type headaches are observed. Despite these headaches, forward angulation may be a benefitial condition for the patient as the neurological symptoms disappear. Instead of not placing anything into the disc space, we believe that the ideal surgical methods are the ones in which the spine arrangement is not destroyed and the disc height is preserved. REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08029f2b.jpg] [gm08029f1b.jpg] [gm08029f1a.jpg] [gm08029f2a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}