 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 5, No. 3, 2008, pp. 170-177 Short-term Prognostic Value Of Rest Tc99m-mibi Gated Spect After Acute Non-q Wave Myocardial Infarction Eser Kaya1, Emre Entok2, Yüksel Cavusoglu3, Hayrettin Saglam4, Erkan Vardareli5, Bilgin Timuralp3 Afyon Kocatepe University Medical Faculty, Departments of Nuclear Medicine1 and Cardiology4, Afyonkarahisar, Osmangazi University Medical Faculty, Departments of Nuclear Medicine2 and Cardiology3, Eskişehir, 5Department of Nuclear Medicine, Acıbadem Hospital, Istanbul, Turkey Code Number: gm08033 Aim: The purpose of this study is to determine the short–term prognostic value of technetium 99m methoxyisobutylisonitrile gated single photon emission computed tomography (Tc99m–MIBI Gated SPECT) in patients with acute Non–Q wave myocardial infarction (NQMI) in 30 days.
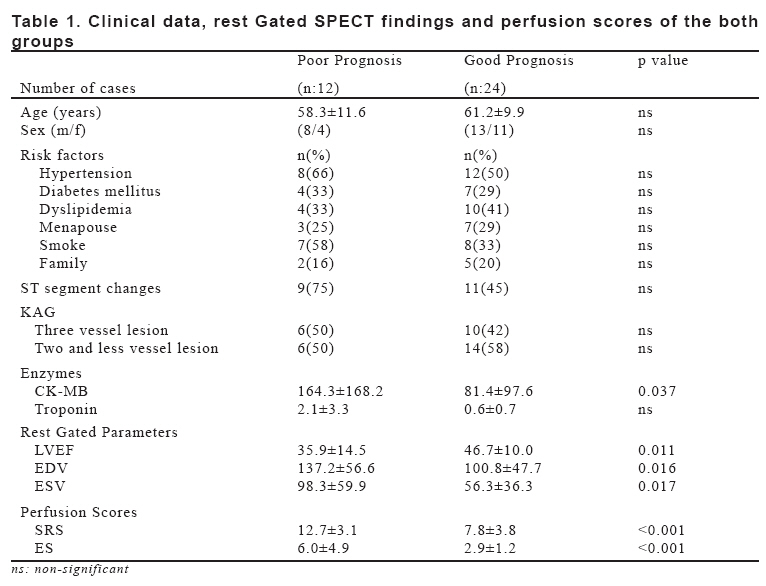
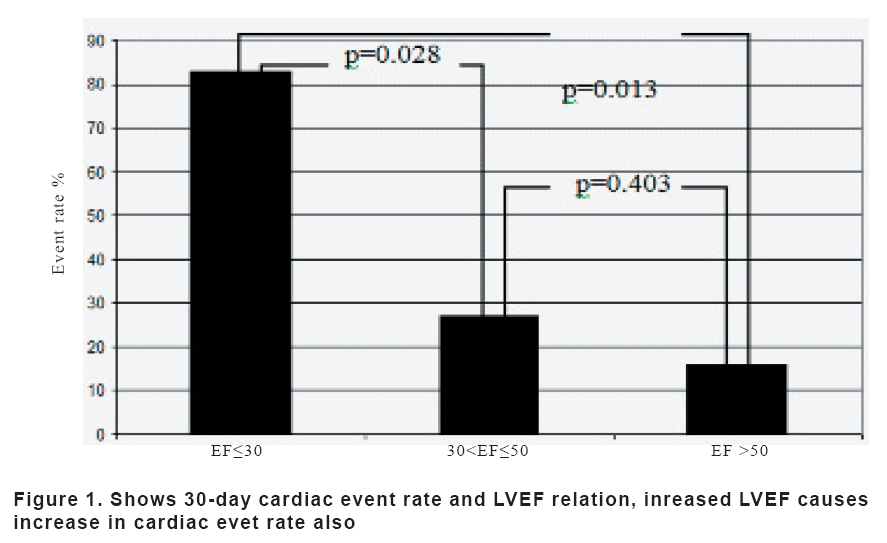
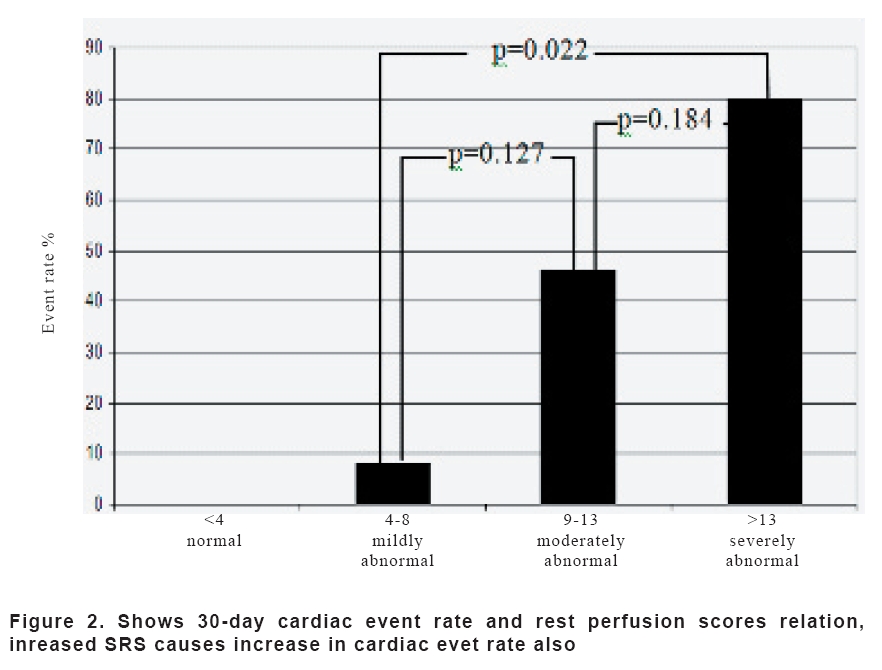
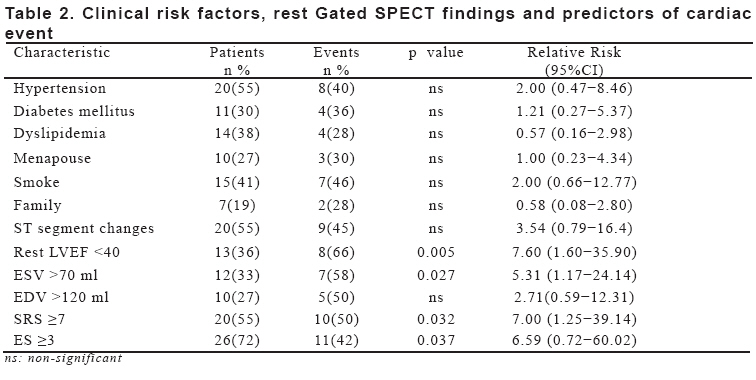
Key words: Non–Q wave myocardial infarction, short–term prognosis, Tc99m–MIBI Gated SPECT. INTRODUCTION Non-Q wave myocardial infarction is characterized by coronary symptoms, elevated cardiac enzyme levels, and ischemic electrocardiographic (ECG) changes without the development of Q waves (1). Although a better initial prognosis, NQMI patients had more frequent infarct extension and reinfarction, resulting in a similar or worse long–term prognosis compared with those with Q wave myocardial infarction (QMI) (2). The investigators in multiple studies have reported the prognostic value of myocardial perfusion imaging in various patient subsets at short–to intermediate–term follow–up (3). Myocardial perfusion data can be clinically useful in the evaluation of patients who have had an acute myocardial infarction (MI) with respect to determining infarct size, assessing the degree of myocardial salvage after reperfusion, determining myocardial viability in infarct zones, and detecting perfusion defect severity (4). In coronary artery disease (CAD) and in patients with recent acute MI, myocardial perfusion single photon emission computed tomography (SPECT) is an effective method for risk stratification (5), diagnosis and prognosis (6). Prognosis of acute MI is also related to the degree of left ventricular dysfunction and extent and severity of CAD (7). Gated SPECT has been a major breakthrough in the practice of nuclear cardiology, and offers important additional prognostic information over that given by perfusion data alone, the possibility to simultaneously assess both myocardial perfusion and left ventricular ejection fraction (LVEF) and left ventricular volumes (8,9). The two most powerful predictors of prognosis (total defect size and resting LVEF) can be assessed with a single test with Gated SPECT (4). The widest experience about the prognostic value of the functional parameters derived from Gated SPECT (8). Technetium 99m (Tc99m) labeled perfusion agents have been introduced into clinical practice to enhance the specificity of SPECT. Methoxyisobutylisonitrile (MIBI) is a lipophylic cation and passes the cell membrane by passive diffusion and also the more favorable physical characteristics of Tc99m imaging with a gamma camera is to obtain better image quality (4). To our knowledge, no finding of short–term prognostic studies involving rest Gated SPECT imaging are currently available. The purpose of our study is to determine the short-term prognostic value of rest Tc99m–MIBI Gated SPECT findings in patients with NQMI. MATERIAL AND METHODS Patient population The study group was consisted of 36 patients (21 males and 15 females), mean age 60.30±10.17 years (range: 37−78). The 20 patients had ST segment changes on the electrocardiography (ECG). NQMI was confirmed by elevation enzymatic data. All patients were identified who had undergone rest Gated SPECT within 48 (30.7±2.3) hours of admission to the coronary care unit. The occurrence of 30 days-with in-hospital-cardiac events was considered in risk stratification. Acquisition protocol Tc99m–MIBI Gated SPECT imaging was performed with a dual–head gamma camera (Marconi Axis 2000 Prism) equipped with a low energy, high resolution collimator (LEHR) and an energy interval of 140±10% keV in a 64x64 matrix. Images were acquired in a 180° orbit with 30s readings every 3°. The R–R interval in the ECG was divided into eight parts. Transverse reconstruction was automatically applied in the quantitative Gated SPECT (QGS) process (ramp filter, 180 filtered BP parallel). In the post–filtering procedure, a low–pass filter order was 5 and the cut–off was 0.21. In the pre-filtering process run before reconstruction in the CEqual analysis (Cedars–Emory quantitative analysis), the low–pass (Butterworth) filter order/cut–off values in rest study was 5/0.25. Image analysis Short–axis images were processed by using Gated SPECT algorithms with the results obtained from Gated SPECT study by quantitative analysis and left ventricular functional parameters [left ventricular ejection fraction (LVEF), end diastolic volume (EDV) and end systolic volume (ESV)], were calculated. Gated projection data sets were converted to summed non–gated data and vertical long axis, horizontal long axis, and short-axis images were reconstructed by CEqual method. This method is highly reproducible and can be used to interpret temporal changes in myocardial perfusion (10,11). Semiquantitative visual interpretation of myocardial perfusion images was done by consensus of two experienced readers without knowledge of specific diagnosis or patient’s identity. Myocardial perfusion was scored using a 17 segment model, on a 0 to 4 scale (0: normal perfusion, 1: mild decrease of photon counts, 2: moderate decrease of photon counts, 3: severe decrease of photon counts, 4: absent photon counts) (12). The summed rest score (SRS) was calculated by adding the scores for all segments, for perfusion defect extent (extent score: ES) was also determined by adding the number of abnormal segments. Coronary Angiography Coronary angiography (CAG) was applied all patients after Gated SPECT study. CAG was performed by Judkin’s technique. The stenosis in the coronary arteries were classified as normal, mild (50–70%) and severe (70–100%) by two cardiologists according to the coronary flow thrombolysis in myocardial infarction classification. Medical record review We assessed clinical risk factors by reviewing the medical record. Clinical variables considered were age, sex, hypertension, diabetes mellitus, dyslipidemia, menapouse, smoke, family, ST segment changes and CAG. The patients were divided into two groups according to their prognosis in which the patients who had new clinical event, were assigned as poor prognosis. And the patients who had well outcome, describe as good prognosis. All clinical data and rest Gated SPECT findings were compared among the two groups (Table 1). Patient follow-up Follow–up was obtained for 30 days–in hospital and after discharge–with a mean of 30.65±0.49 days. Telephone interviews were performed, and hospital charts reviewed and primary physicians contacted for confirmation. Cardiac events included reinfarction, revascularization, congestive heart failure and death. Statistical analysis All parametric results were expressed as mean ± standard deviation for each group. Shapiro–Wilks test was performed to check the normality of the data before running tests. Comparisons of the between groups subjects were performed using the t test and Mann-whitney U test. Chi–square and Fisher’s Exact test were performed nonparametric results. Relative risk (RR) with 95% confidence intervals (CI) was calculated by logistic regression analysis. The relative risk with the 95% confidence intervals (CI) are presented. A p–value less than 0.05 was considered to be statistically significant. RESULTS During the follow-up period (include hospitalization) (30.65±0.49 day), 12 patients (33%) had a new clinical event, (4 congestive heart failure (11%), 7 revascularization (19%), 1 reinfarct (2%) and no death), whereas 24 patients (66%) showed a good outcome. Clinical data and rest Gated SPECT findings in patients with short–term prognosis are shown in Table 1. There were no stastistical differances in age, sex, risk factors, ST segment changes, and CAG result (two or three vessel lesion) between two groups. Creatine Kinase–Myocardial Binding (CK–MB) enzyme levels were significantly different in two groups (p=0.037) and troponin levels were not different. There were significant differences in LVEF, EDV, ESV, SRS and ES values between poor and good prognosis group (p=0.011, p=0.016, p=0.017, p<0.001, p<0.001, respectively). The relationships between scintigraphic quantitative paramaters (EF, SRS) and cardiac event rate are shown in figures 1 and 2. By univariate analysis, Gated SPECT parameters; Rest LVEF<40% (RR= 7.66, CI 1.60 to 35.90), ESV>70 ml (RR=5.31, CI 1.17 to 24.14), SRS≥7 (RR=7.00, CI 1.25 to 39.14) and ES≥3 (RR=6.59 CI 0.72 to 60.02) were predictors of cardiac events (Table 2). DISCUSSION Although left ventricular functions are protected by perfusional alterations in subendocardial area in NQMI patients, the ratio of possible new cardiac events are almost the same (13). Patients with an acute MI may be benefit from simultaneous evaluation of left ventricular function and myocardial perfusion using Gated SPECT imaging because both LVEF and perfusion defect size are prognostically important (14). LVEF and measurement of left ventricular volumes have important clinical implications for prognosis of patients with cardiac disease (15), and those paramaters are powerful independent prognostic variables (16). Multiple studies have shown that resting and exercise LVEF, measured by radionuclide methods, are powerful predictors of cardiac events (17), and have incremental prognostic value in patients with acute MI (18). But, the functional parameters obtained using a post–stress Gated SPECT can be partly influenced by the presence of post–ischemic stunning and thus should be considered slightly different from a true resting LVEF (8). The first and most obvious prognostic parameter is the resting LVEF, this parameter has a predictive value for the development of heart failure, cardiac death and hard events in patients with a first non–complicated myocardial infarction (8,18). In this study, rest EF was a most powerful predictor of all cardiac events, and the patients with congestive heart failure had EF less than 30. Various investigators have used different LVEF (30%-50%, EF) values for determining risk stratification and prognosis (4,19,20,21). All of these studies were about middle–long term prognosis and risk stratification. We could not found any study in the literature about short-term risk stratification and prognosis on NQMI using rest Tc99m–MIBI GATED SPECT to make a comparison with our findings. We think that our study is a preliminary study that showed the short term prognosis of NQMI patients by performing Tc99m–MIBI Gated SPECT. In our study; new cardiac event rate was 66%, this results in a hazard ratio of 7.6 for patients with a LVEF lower than 40% (CI 1.60 to 35.90). Other indicators of high risk; increased EDV and ESV in CAD (22). Sharir et al. (17) described; threshold values for ESV: 70 ml and EDV: 120ml for prognosis, and showed that an ESV>70 ml was related to high death rate in patients with mild–to–moderate or severe perfusion defect in CAD. The annual cardiac mortality rate was 10.4 % in patients with a resting end-systolic volume greater than 70 ml, resulting in a hazard ratio of 4.5 (23). In our sudy, with the ESV>70 ml and mild–to–severe perfusion defects of patients had no death but new cardiac event rate was 100%, with a hazard ratio of 5.31 (CI 1.17 to 24.14, p=0.027). If EDV>120 ml is high risk for cardiac death (17), in our study; new cardiac event rate was 50% in the patients with EDV>120 ml. Hachamovitch et al. (24) showed the enhanced prognostic value of myocardial perfusion imaging. Multiple perfusion abnormalities (large perfusion defect size), multi–vessel disease scan pattern with defects in two or more vascular supply regions, shows high–risk myocardial perfusion scan variables after acute MI (4,6). Mildly abnormal perfusion studies are associated with a low risk of cardiac death or myocardial infarction, whereas markedly abnormal scans are associated with a high risk of cardiac events (24). Patients with normal images or small defects have a significantly better outcome than patients with abnormal images or large defects (14). Iskandrian et al. (25) found that the total number of myocardial perfusion defects was the single best predictor of subsequent event, and both extent and severity of hypoperfusion were exponentially correlated with event rate. Similar in our study; increased severity and extent of perfusion defect caused increased cardiac event rate . Sharir et al. (26) the prediction of cardiac death demonstrated that the most powerful predictor was the SRS in randomize patients who had myocardial perfusion SPECT. In a study; the value of SRS was higher at cardiac death compared to MI at the patient who had SPECT study (24). Douglas et al. (27) stated that cardiac event rate is higher in patients with perfusion defect score over 7. In our study, the patients, whose SRS was greater than 7, had a 50% cardiac event and relative risk was 7.00 with CI 1.25 to 39.14 in 30 days, and severity and extent of perfusion defect were a predictor for new cardiac event, SRS was more predictive than ES. As another word, increased the severity of perfusion defect, increased the probability of new cardiac events for NQMI in 30 days. According to Sharir et al. (17); the perfusion data were superior to function in predicting total events, whereas function data were superior to perfusion in predicting cardiac death. The greater impact of perfusion compared with function information on early referral for revascularization and on the crossover of patients from medical to revascularization treatment may account for the higher prognostic power of EF and ESV in the prediction of cardiac death compared with perfusion information, because patients with significant perfusion abnormalities are referred for aggressive treatment. Further incorporation of Gated SPECT data (EF and ESV) into the decision process of referral for revascularization may result in a reduction of the cardiac death rate (17). The event rate increased with decreased EF and with increased ESV, SRS and ES (18). In our study, LVEF<40%, increased EDV, ESV, SRS and ES were related high cardiac event, functional data (EF, ESV) were superior in predicting all cardiac event. The prognostic value of the resting LVEF and ESV had a higher predictive value for all cardiac event than SRS and ES (p=0.005, p=0.027, p=0.032, p=0.037, respectively). Patients with EF<40% / resting perfusion defects / increased EDV and ESV, have a higher risk of multivessel CAD and have worse clinical outcomes (6). The event rate increased with decreasing values of EF and with increasing values of rest perfusion and ischemic scores (18). In our study; cardiac event rate was increased in these patients, but cardiac event rate of the patient with three vessel lesions was more less than the patients with two or more less vessel lesion on CAG. The presence of ST segment changes and elevations of troponin and CK–MB are objective correlates of advers short–and long–term prognosis with NQMI (28). In our study, in 45% of patients with ST segment alteration had new cardiac event and the patients with higher levels of CK-MB had poor short term prognosis. Study Limitations; The use of left ventricular ejection fraction measurement as a predictor of outcome in the very early acute phase of myocardial infarction has some limitations. Some patients may demonstrate substantial hyperkinesis of the normally perfused zone, which influences global performance to some degree. This may falsely rise the left ventricular ejection fraction. However, large scale study is needed for obtaining reliable outcomes for determination of short–term prognosis in patients with NQMI. In conclusion, the main findings from the our study; left ventricular parameters (EF, ESV) and perfusion scores (SRS, ES) which obtained by rest Tc99m–MIBI Gated SPECT, provide useful information for short–term prognosis after NQMI in 30 days. This study demonstrates poor prognosis related decreased LVEF, increased ESV, SRS and ES. The prognostic value of the resting LVEF and ESV had a higher predictive value for all cardiac event than either perfusion SPECT or clinical parameters, and SRS and ES nearly these parameters. Acknowledgment The research reported here was presented at the 8th International Conference of Nuclear Cardiology, Prague, Czech Republic, 29 April−2 May 2007. REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08033t1.jpg] [gm08033f2.jpg] [gm08033t2.jpg] [gm08033f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}