 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
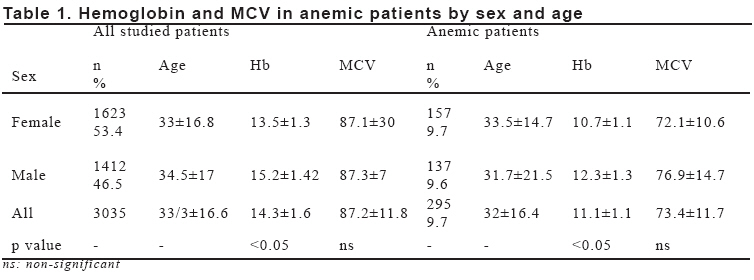
European Journal of General Medicine, Vol. 5, No. 3, 2008, pp. 178-180 Hypochromic Microcytic Anemia In Northwestern Of Tabriz, Iran Susan Kolahi, Halea Farzin, Manouchehr Khoshbaten Tabriz University, Faculty of Medicine, Drug Applied Research Center, Tabriz, Iran Code Number: gm08034 Aim: Hypochromic microcytic anemia included iron Deficiency Anemia (IDA) and thalassemia is a worldwide problem with easy treatment and important unwanted symptoms that widely prevalent in Iran.
Key words: Anemia, hypochromic microcytic anemia, Iron deficiency anemia, minor thalassemia, Iran INTRODUCTION Iron deficiency anemia (IDA) has worldwide prevalence (1). IDA has 5% prevalence in the world , but in developing country it is 18% among adult women and 10% in adult men (2,3,6). IDA is an end stage of negative iron balance. It is preceded by a stage of latent iron deficiency (ID) where serum ferritin is below 15.0 ng/ml with normal Hb level (4). It would be interesting to see the prevalence of ID in addition to IDA. Mild anemia is asymptomatic or cause non-specific symptoms. In IDA, besides Hb, MCV and MCH are also reduced. In recent years the prevalence of IDA reduced in Iran because of early diagnosis and early and cheap iron therapy. Thalassemia is a congenital disease; Iran lies on thalassemic region of the world, and the prevalence of thalasemia is 2.3% in Iran (5). Anemia causes paleness, heart palpitation, tinnitus, headache, agitation and fatigue (2,6). Upon these unwanted symptoms of anemia and the high prevalence of this disease in Iran we used to report the prevalence of hypochromic microcytic anemia in Iran. Women were already anemic at the time of conception, with an estimated prevalence of anemia of 43% in nonpregnant women in developing countries and of 12% in women in wealthier regions (7). MATERIAL AND METHODS 3035 households (1623 female and 1412 male) were studied after obtaining their informed consent. None of subjects involved in the study had been on any hematinic drugs in last six months or had any infection in past one month. A questionnaire was given to assess symptoms due to anemia. Arbitrary score was assigned according to the response to the questionnaire. Citrated blood samples were being assessed with Technican H1 (USA) for Hb, Hct and MCV. If Hb in male were being under 13.5 mg/dlit or being under 12 mg/dlit in non pregnant female, we get 5cc blood to assess their serum iron, TIBC, ferritin and retic count .Serum iron, TIBC and ferritin were being analyzed by Tris kit (Australia) and Hitachi 704 autoanalyser system (Germany) in referral laboratory. If there wasn’t any evidence of IDA; blood samples with MCV under 80 were being studied for Hb electrophoresis with Hellena kits in Hellena set (France). Whenever blood sample’s Ferritin was under 15nanogram/millit we defined them as IDA (1). Minor thalassemia defined as Hb A2 up to two folds or higher, or increasing of HbF (5). RESULTS 3035 of households completed the study and were available for repeat blood test. Data of these 3035 subjects was analyzed. 1623 (53.4%) subjects were female. Mean age was 33 years (range 16-49). 1412 subjects were male (46.5%). 9.7% of understudy people were anemic. Results of baseline studies are shown in Table 1. Prevalence of IDA and minor thalassemia in female and IDA and minor thalassemia in male were 7%,1%, 2% and 5%, respectively. Among patients who categorized as IDA, in 82% of these patients MCV was under 80 and 56% of them were infected by parasites. In female who categorized as IDA, mean of ferritin was 6.1±2.8 and in male was 5.1±1.8. Transferin saturation percent was less than 16% in 87.3% of IDA patients and was more than 16% in 12.6% of them. Only in 1.2 % of subjects MCV was lower than 80 without any evidence of IDA or thalasemia; but 34% of these patients had hypoferritinemia; and in the rest of them we couldn’t find any reason. In all patients with minor thalassemia MCV/RBC index was lower than 13. DISCUSSION In this study the prevalence of anemia was 9.7% in male and female who had entered the study. In one study the prevalence of anemia was 11.5% (12.7% in female and 10% in male) and in 90% of cases the IDA was the reason of anemia (2). In our study prevalence of IDA and minor thalassemia in female and IDA in and minor thalassemia in male were 7%,1%, 2% and 5%, respectively. This study conclude that IDA was the reason of 75% of anemia. Existing the following study by men more than women might be the reason of the high prevalence of thalassemia in this study. Only in 82% of IDA patients MCV was lower than 80 and in all thalassemic patients MCV/RBC index was lower than 13; these findings was in agree with that was in previous study (8,9,10). In 87.3% of IDA patients transferrine saturation percent was lower than 16. As point as different theories about the relationships between transferrin saturation percent and IDA ;there isn’t high specificity for transferrine saturation percent test to determine IDA (11). On the other hand, iron deficiency is widespread among females in Iran as shown by this study; but anemia decreases, perhaps due to hematinic therapy like other countries. Then this problem must be overemphasized by public health system, because of too easy and available treatment and nutrition education for people. Our people don’t know that which foods to eat and what foods help their health. REFERENCES
Copyright 2008 - European Journal of General Medicine The following images related to this document are available:Photo images[gm08034t1.jpg] |
| |||||||||

{kind=link}